Papadimos Thomas J, Habib Robert H, Zacharias Anoar, Schwann Thomas A, Riordan Christopher J, Durham Samuel J, Shah Aamir
Department of Anesthesiology, Medical College of Ohio, 3000 Arlington Avenue, Toledo, OH 43614, USA.
BMC Surg. 2005 May 2;5:10. doi: 10.1186/1471-2482-5-10.
The Leapfrog Group recommended that coronary artery bypass grafting (CABG) surgery should be done at high volume hospitals (>450 per year) without corresponding surgeon-volume criteria. The latter confounds procedure-volume effects substantially, and it is suggested that high surgeon-volume (>125 per year) rather than hospital-volume may be a more appropriate indicator of CABG quality.
We assessed 3-year isolated CABG morbidity and mortality outcomes at a low-volume hospital (LVH: 504 cases) and compared them to the corresponding Society of Thoracic Surgeons (STS) national data over the same period (2001-2003). All CABGs were performed by 5 high-volume surgeons (161-285 per year). "Best practice" care at LVH -- including effective practice guidelines, protocols, data acquisition capabilities, case review process, dedicated facilities and support personnel -- were closely modeled after a high-volume hospital served by the same surgeon-team.
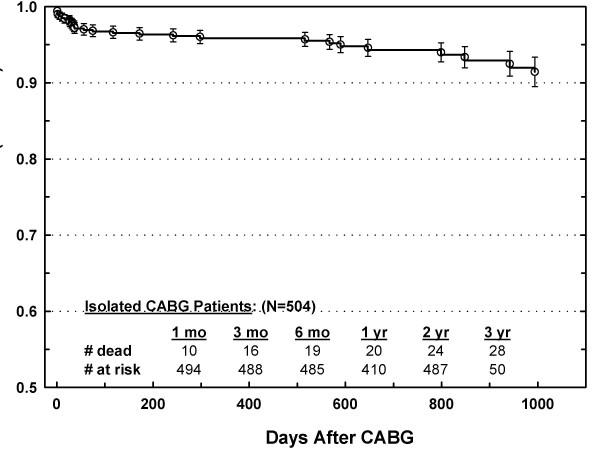
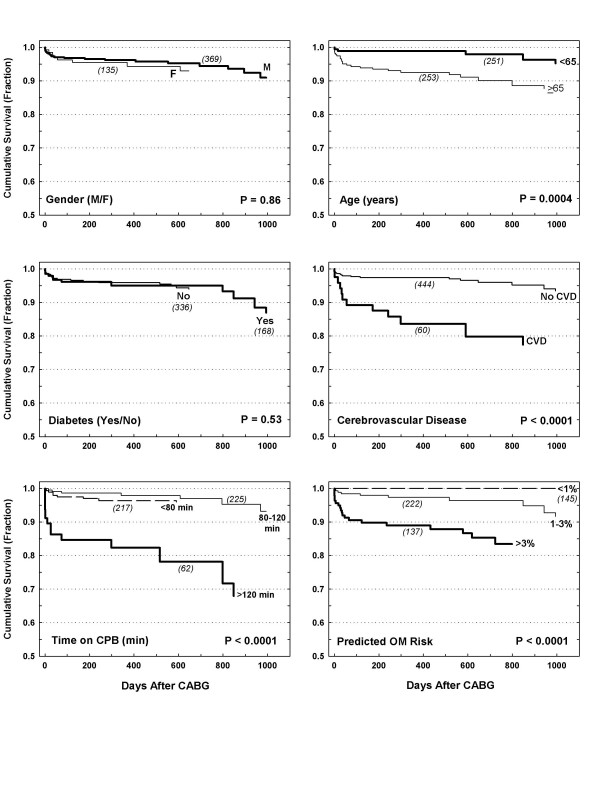
Operative mortality was similar for LVH and STS (OM: 2.38% vs. 2.53%), and the corresponding LVH observed-to-expected mortality (O/E = 0.81) indicated good quality relative to the STS risk model (O/E<1). Also, these results were consistent irrespective of risk category: O/E was 0, 0.9 and 1.03 for very-low risk (<1%), low risk (1-3%) and moderate-to-high risk category (>3%), respectively. Postoperative leg wound infections, ventilator hours, renal dysfunction (no dialysis), and atrial fibrillation were higher for LVH, but hospital stay was not. The unadjusted Kaplan-Meier survival for the LVH cohort was 96%, 94%, and 92% at one, two, and three years, respectively.
Our results demonstrated that high quality CABG care can be achieved at LVH programs if 1) served by high volume surgeons and 2) patient care procedures similar to those of large programs are implemented. This approach may prove a useful paradigm to ensure high quality CABG care and early efficacy at low volume institutions that wish to comply with the Leapfrog standards.
“跨越组织”建议冠状动脉搭桥术(CABG)应在每年手术量高的医院(>450例/年)进行,而未设定相应的外科医生手术量标准。后者极大地混淆了手术量的影响,有人认为外科医生年手术量高(>125例/年)而非医院手术量可能是CABG质量更合适的指标。
我们评估了一家低手术量医院(LVH:504例病例)3年单纯CABG的发病率和死亡率结果,并将其与同期(2001 - 2003年)相应的胸外科医师协会(STS)全国数据进行比较。所有CABG手术均由5位高手术量外科医生(每年161 - 285例)实施。LVH的“最佳实践”护理——包括有效的实践指南、方案、数据采集能力、病例审查流程、专用设施和支持人员——紧密仿照由同一外科医生团队服务的高手术量医院。
LVH和STS的手术死亡率相似(OM:2.38%对2.53%),相应的LVH观察到的与预期的死亡率(O/E = 0.81)相对于STS风险模型(O/E<1)表明质量良好。此外,无论风险类别如何,这些结果都是一致的:极低风险(<1%)、低风险(1 - 3%)和中高风险类别(>3%)的O/E分别为0、0.9和1.03。LVH的术后腿部伤口感染、呼吸机使用时长、肾功能不全(无需透析)和房颤发生率较高,但住院时间并非如此。LVH队列未调整的Kaplan - Meier生存率在1年、2年和3年分别为9