Watson Nicholas F S, Madjd Zahra, Scrimegour Duncan, Spendlove Ian, Ellis Ian O, Scholefield John H, Durrant Lindy G
Academic Department of Clinical Oncology, University of Nottingham, City Hospital, Nottingham, NG5 1PB, UK.
World J Surg Oncol. 2005 Jul 19;3:47. doi: 10.1186/1477-7819-3-47.
Advances in our understanding of the molecular biology of colorectal cancer have fuelled the search for novel molecular prognostic markers to complement existing staging systems. Markers assessed in combination may perform better than those considered individually. Using high-throughput tissue microarray technology, we describe the prognostic value of combined p53 / Bcl-2 status in colorectal cancer.
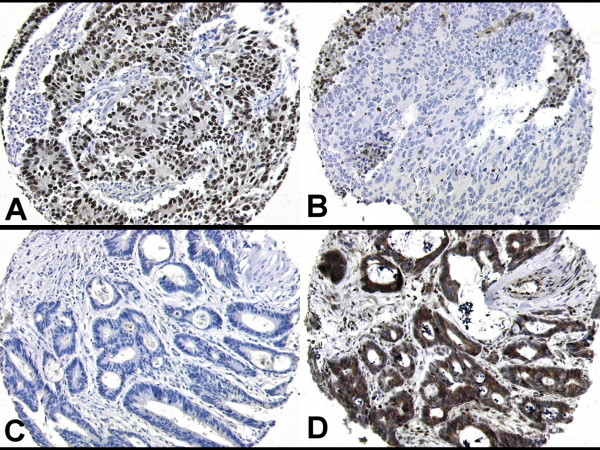
Tumour samples from 462 patients who underwent elective surgery to resect a primary colorectal cancer between 1994 and 2000 (mean follow-up of 75 months) were assembled in tissue microarray format. Clinico-pathological data including tumour grade, stage, vascular invasion status along with disease specific survival data has been collected prospectively. Immunohistochemical analysis of p53 and Bcl-2 expression was performed using antibodies DO-7 (p53) and 124 (Bcl-2), and results correlated with known clinico-pathological variables and outcomes.
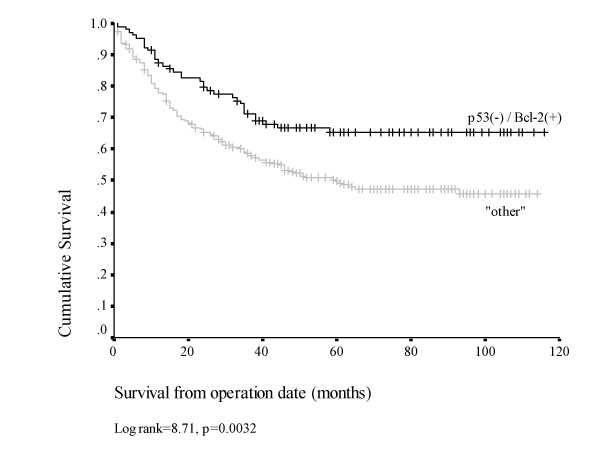
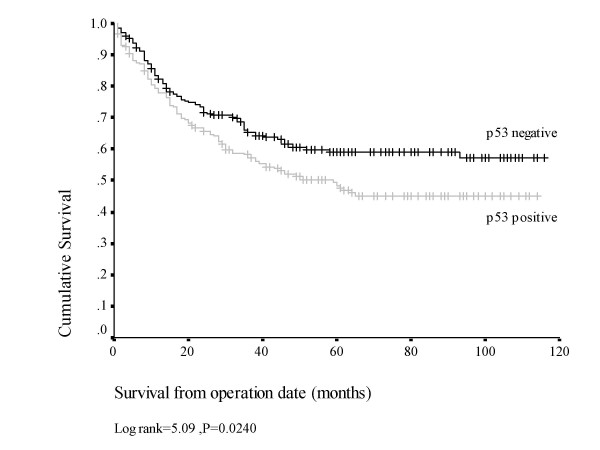
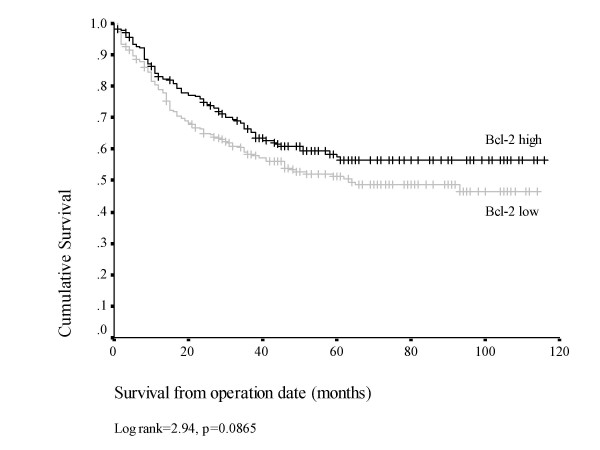
Abnormal nuclear p53 accumulation and Bcl-2 overexpression were detected in 221/445 (49.6%) and199/437 (45.5%) tumours respectively, with a significant inverse correlation between the two markers (p = 0.023). On univariate analysis no correlations were found between either marker and standard clinico-pathological variables, however nuclear p53 expression was associated with a significantly reduced survival (p = 0.024). Combined analysis of the two markers indicated that 112/432 (24.2%) cases displayed a p53(-)/Bcl-2(+) phenotype, this occurring more frequently in earlier stage tumours. Kaplan-Meier analysis revealed a significant survival advantage in these p53(-)/Bcl-2(+) tumours compared with the remaining cases (p = 0.0032). On multivariate analysis using the Cox proportional hazards model, neither p53 expression nor Bcl-2 expression alone were of independent prognostic significance, however the combined p53(-)/Bcl-2(+) phenotype was significantly associated with a good prognosis in this series (HR 0.659, 95%CI 0.452-0.959, p = 0.029).
Patient stratification by combined p53 / Bcl-2 phenotype provides stage-independent prognostic information in colorectal cancer. Specifically, that up to a quarter of patients display a good prognosis p53(-)/Bcl-2(+) phenotype. This may indicate a more clinically indolent phenotype and a subset of patients for whom less aggressive adjuvant treatment appropriate.
我们对结直肠癌分子生物学认识的进展推动了对新型分子预后标志物的探索,以补充现有的分期系统。联合评估的标志物可能比单独考虑的标志物表现更好。我们使用高通量组织微阵列技术描述了结直肠癌中联合p53 / Bcl-2状态的预后价值。
收集了1994年至2000年间接受择期手术切除原发性结直肠癌的462例患者的肿瘤样本(平均随访75个月),制成组织微阵列形式。前瞻性收集了包括肿瘤分级、分期、血管侵犯状态以及疾病特异性生存数据等临床病理资料。使用DO-7(p53)和124(Bcl-2)抗体对p53和Bcl-2表达进行免疫组化分析,结果与已知的临床病理变量和结局相关。
分别在221/445(49.6%)和199/437(45.5%)的肿瘤中检测到异常核p53积累和Bcl-2过表达,两种标志物之间存在显著负相关(p = 0.023)。单因素分析未发现任何一种标志物与标准临床病理变量之间存在相关性,然而核p53表达与生存率显著降低相关(p = 0.024)。两种标志物的联合分析表明,112/432(24.2%)的病例表现为p53(-)/Bcl-2(+)表型,这种情况在早期肿瘤中更常见。Kaplan-Meier分析显示,与其余病例相比,这些p53(-)/Bcl-2(+)肿瘤具有显著的生存优势(p = 0.0032)。使用Cox比例风险模型进行多因素分析时,单独的p53表达和Bcl-2表达均无独立的预后意义,然而联合的p53(-)/Bcl-2(+)表型在本系列中与良好预后显著相关(HR 0.659,95%CI 0.452 - 0.959,p = 0.029)。
根据联合p53 / Bcl-2表型对患者进行分层可为结直肠癌提供独立于分期的预后信息。具体而言,高达四分之一的患者表现出预后良好的p53(-)/Bcl-2(+)表型。这可能表明一种临床上更惰性的表型,以及一部分适合采用侵袭性较小的辅助治疗的患者。