Ratanarat Ranistha, Brendolan Alessandra, Piccinni Pasquale, Dan Maurizio, Salvatori Gabriella, Ricci Zaccaria, Ronco Claudio
Department of Nephrology, Dialysis and Transplantation, St Bortolo Hospital, Vicenza, Italy.
Crit Care. 2005 Aug;9(4):R294-302. doi: 10.1186/cc3529. Epub 2005 Apr 28.
Severe sepsis is the leading cause of mortality in critically ill patients. Abnormal concentrations of inflammatory mediators appear to be involved in the pathogenesis of sepsis. Based on the humoral theory of sepsis, a potential therapeutic approach involves high-volume haemofiltration (HVHF), which has exhibited beneficial effects in severe sepsis, improving haemodynamics and unselectively removing proinflammatory and anti-inflammatory mediators. However, concerns have been expressed about the feasibility and costs of continuous HVHF. Here we evaluate a new modality, namely pulse HVHF (PHVHF; 24-hour schedule: HVHF 85 ml/kg per hour for 6-8 hours followed by continuous venovenous haemofiltration 35 ml/kg per hour for 16-18 hours).
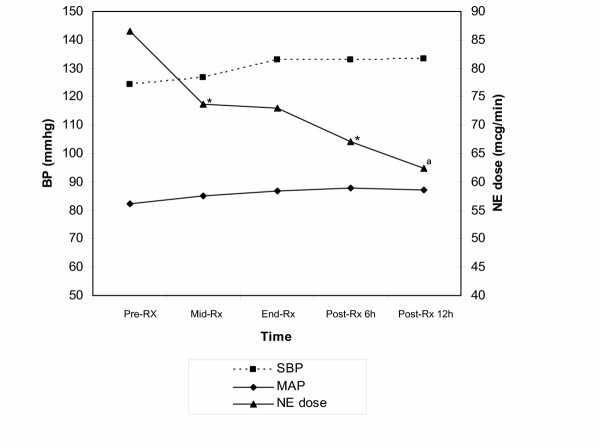
Fifteen critically ill patients (seven male; mean Acute Physiology and Chronic Health Evaluation [APACHE] II score 31.2, mean Simplified Acute Physiology Score [SAPS] II 62, and mean Sequential Organ Failure Assessment 14.2) with severe sepsis underwent daily PHVHF. We measured changes in haemodynamic variables and evaluated the dose of noradrenaline required to maintain mean arterial pressure above 70 mmHg during and after pulse therapy at 6 and 12 hours. PHVHF was performed with 250 ml/min blood flow rate. The bicarbonate-based replacement fluid was used at a 1:1 ratio in simultaneous pre-dilution and post-dilution.
No treatment was prematurely discontinued. Haemodynamics were improved by PHVHF, allowing a significant reduction in noradrenaline dose during and at the end of the PHVHF session; this reduction was maintained at 6 and 12 hours after pulse treatment (P = 0.001). There was also an improvement in systolic blood pressure (P = 0.04). There were no changes in temperature, cardiac index, oxygenation, arterial pH or urine output during the period of observation. The mean daily Kt/V was 1.92. Predicted mortality rates were 72% (based on APACHE II score) and 68% (based on SAPS II score), and the observed 28-day mortality was 47%.
PHVHF is a feasible modality and improves haemodynamics both during and after therapy. It may be a beneficial adjuvant treatment for severe sepsis/septic shock in terms of patient survival, and it represents a compromise between continuous renal replacement therapy and HVHF.
严重脓毒症是重症患者死亡的主要原因。炎症介质浓度异常似乎参与了脓毒症的发病机制。基于脓毒症的体液学说,一种潜在的治疗方法是高容量血液滤过(HVHF),它已在严重脓毒症中显示出有益效果,可改善血流动力学并非选择性地清除促炎和抗炎介质。然而,人们对持续HVHF的可行性和成本表示担忧。在此,我们评估一种新的模式,即脉冲式HVHF(PHVHF;24小时方案:每小时85 ml/kg的HVHF持续6 - 8小时,随后每小时35 ml/kg的持续静静脉血液滤过持续16 - 18小时)。
15例患有严重脓毒症的重症患者(7例男性;急性生理学与慢性健康状况评估[APACHE] II评分平均为31.2,简化急性生理学评分[SAPS] II平均为62,序贯器官衰竭评估平均为14.2)接受每日PHVHF治疗。我们测量了血流动力学变量的变化,并评估了在脉冲治疗6小时和12小时期间及之后维持平均动脉压高于70 mmHg所需的去甲肾上腺素剂量。PHVHF以250 ml/min的血流速度进行。基于碳酸氢盐溶液的置换液以1:1的比例用于同步前稀释和后稀释。
没有治疗被过早终止。PHVHF改善了血流动力学,使得在PHVHF治疗期间及结束时去甲肾上腺素剂量显著降低;这种降低在脉冲治疗后6小时和12小时仍保持(P = 0.001)。收缩压也有所改善(P = 0.04)。在观察期间,体温、心脏指数、氧合、动脉pH值或尿量没有变化。平均每日Kt/V为1.92。预测死亡率为72%(基于APACHE II评分)和68%(基于SAPS II评分),观察到的28天死亡率为47%。
PHVHF是一种可行的模式,在治疗期间及之后均能改善血流动力学。就患者生存而言,它可能是严重脓毒症/感染性休克的一种有益辅助治疗方法,并且它代表了持续肾脏替代治疗和HVHF之间的一种折衷方案。