Yimer Solomon, Bjune Gunnar, Alene Getu
Amhara National Regional State Health Bureau, Bahir Dar, Ethiopia.
BMC Infect Dis. 2005 Dec 12;5:112. doi: 10.1186/1471-2334-5-112.
Delayed diagnosis and treatment of tuberculosis (TB) results in severe disease and a higher mortality. It also leads to an increased period of infectivity in the community. The objective of this study was to determine the length of delays, and analyze the factors affecting the delay from onset of symptoms of pulmonary tuberculosis (PTB) until the commencement of treatment.
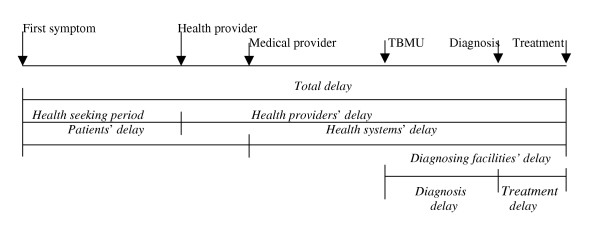
In randomly selected TB management units (TBMUs), i.e. government health institutions which have diagnosing and treatment facilities for TB in Amhara Region, we conducted a cross sectional study from September 1-December 31/2003. Delay was analyzed from two perspectives, 1. Period between onset of TB symptoms to first visit to any health provider (health seeking period), and from the first health provider visit to initiation of treatment (health providers' delay), and 2. Period between onset of TB symptoms to first visit to a medical provider (patients' delay), and from this visit to commencement of anti-TB treatment (health systems' delay). Patients were interviewed on the same date of diagnosis using a semi-structured questionnaire. Logistics regression analysis was applied to analyze the risk factors of delays.
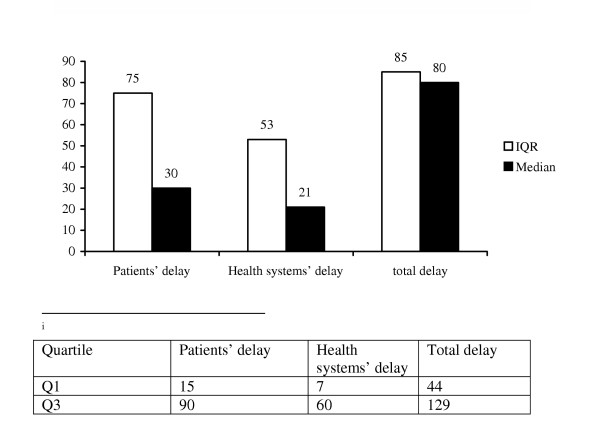
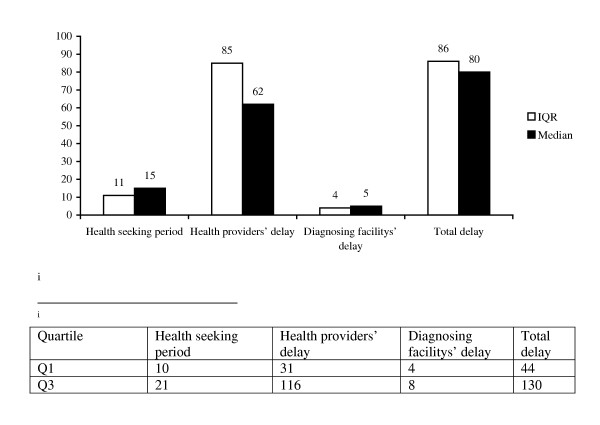
A total of 384 new smear positive PTB patients participated in the study. The median total delay was 80 days. The median health-seeking period and health providers' delays were 15 and 61 days, respectively. Conversely, the median patients' and health systems' delays were 30 and 21 days, respectively. Taking medical providers as a reference point, we found that forty eight percent of the subjects delayed for more than one month. Patients' delays were strongly associated with first visit to non-formal health providers and self treatment (P < 0.0001). Prior attendance to a health post/clinic was associated with increased health systems' delay (p < 0.0001).
Delay in the diagnosis and treatment of PTB is unacceptably high in Amhara region. Health providers' and health systems' delays represent the major portion of the total delay. Accessing a simple and rapid diagnostic test for TB at the lowest level of health care facility and encouraging a dialogue among all health providers are imperative interventions.
结核病(TB)的延迟诊断和治疗会导致严重疾病和更高的死亡率。这也会导致社区内传染期延长。本研究的目的是确定延迟的时长,并分析从肺结核(PTB)症状出现到开始治疗这段延迟的影响因素。
在随机选择的结核病管理单位(TBMUs),即阿姆哈拉地区具备结核病诊断和治疗设施的政府卫生机构中,我们于2003年9月1日至12月31日进行了一项横断面研究。从两个角度分析延迟情况,1. 从结核病症状出现到首次就诊于任何医疗服务提供者的时间段(就医寻求期),以及从首次就诊于医疗服务提供者到开始治疗的时间段(医疗服务提供者延迟),2. 从结核病症状出现到首次就诊于医疗人员的时间段(患者延迟),以及从这次就诊到开始抗结核治疗的时间段(卫生系统延迟)。在诊断当天使用半结构化问卷对患者进行访谈。应用逻辑回归分析来分析延迟的风险因素。
共有384例新的涂片阳性PTB患者参与了本研究。总延迟的中位数为80天。就医寻求期和医疗服务提供者延迟的中位数分别为15天和61天。相反,患者延迟和卫生系统延迟的中位数分别为30天和21天。以医疗人员为参照点,我们发现48%的受试者延迟超过一个月。患者延迟与首次就诊于非正规医疗服务提供者和自我治疗密切相关(P<0.0001)。之前到卫生站/诊所就诊与卫生系统延迟增加相关(P<0.0001)。
在阿姆哈拉地区,PTB诊断和治疗的延迟高得令人无法接受。医疗服务提供者延迟和卫生系统延迟占总延迟的主要部分。在最低级别的医疗保健机构提供简单快速的结核病诊断检测,并鼓励所有医疗服务提供者之间进行沟通,是必要的干预措施。