Luecke Thomas, Pelosi Paolo
Department of Anesthesiology and Critical Care Medicine, University Hospital of Mannheim, Germany.
Crit Care. 2005;9(6):607-21. doi: 10.1186/cc3877. Epub 2005 Oct 18.
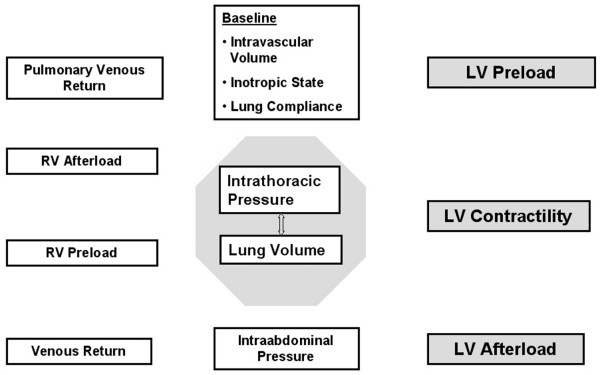
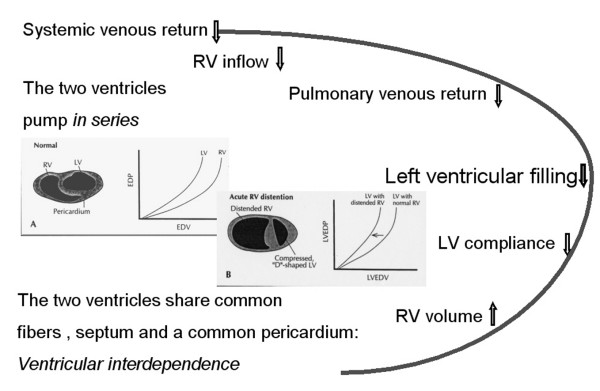
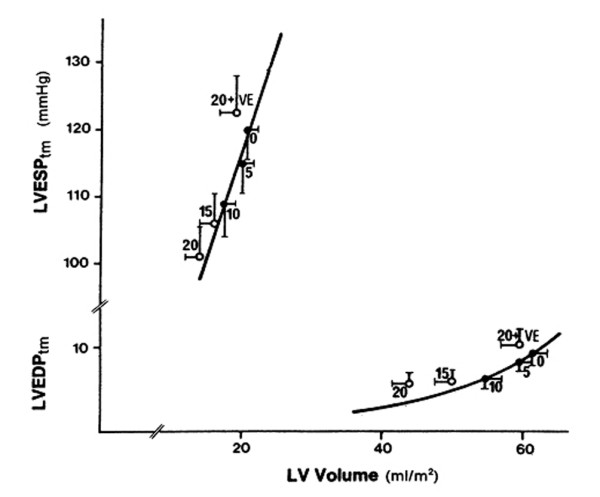
In patients with acute lung injury, high levels of positive end-expiratory pressure (PEEP) may be necessary to maintain or restore oxygenation, despite the fact that 'aggressive' mechanical ventilation can markedly affect cardiac function in a complex and often unpredictable fashion. As heart rate usually does not change with PEEP, the entire fall in cardiac output is a consequence of a reduction in left ventricular stroke volume (SV). PEEP-induced changes in cardiac output are analyzed, therefore, in terms of changes in SV and its determinants (preload, afterload, contractility and ventricular compliance). Mechanical ventilation with PEEP, like any other active or passive ventilatory maneuver, primarily affects cardiac function by changing lung volume and intrathoracic pressure. In order to describe the direct cardiocirculatory consequences of respiratory failure necessitating mechanical ventilation and PEEP, this review will focus on the effects of changes in lung volume, factors controlling venous return, the diastolic interactions between the ventricles and the effects of intrathoracic pressure on cardiac function, specifically left ventricular function. Finally, the hemodynamic consequences of PEEP in patients with heart failure, chronic obstructive pulmonary disease and acute respiratory distress syndrome are discussed.
在急性肺损伤患者中,尽管“激进”的机械通气会以复杂且通常不可预测的方式显著影响心脏功能,但可能仍需要高水平的呼气末正压(PEEP)来维持或恢复氧合。由于心率通常不会随PEEP而改变,心输出量的整体下降是左心室每搏输出量(SV)减少的结果。因此,根据SV及其决定因素(前负荷、后负荷、收缩力和心室顺应性)的变化来分析PEEP引起的心输出量变化。与任何其他主动或被动通气操作一样,PEEP机械通气主要通过改变肺容积和胸内压来影响心脏功能。为了描述需要机械通气和PEEP的呼吸衰竭的直接心脏循环后果,本综述将重点关注肺容积变化的影响、控制静脉回流的因素、心室之间的舒张期相互作用以及胸内压对心脏功能(特别是左心室功能)的影响。最后,讨论了PEEP对心力衰竭、慢性阻塞性肺疾病和急性呼吸窘迫综合征患者的血流动力学后果。