Andriesse Gunnar I, Verhoef Jan
Eijkman-Winkler Institute for Medical and Clinical Microbiology, University Medical Center Utrecht (UMCU), Utrecht, The Netherlands.
Treat Respir Med. 2006;5(1):11-30. doi: 10.2165/00151829-200605010-00002.
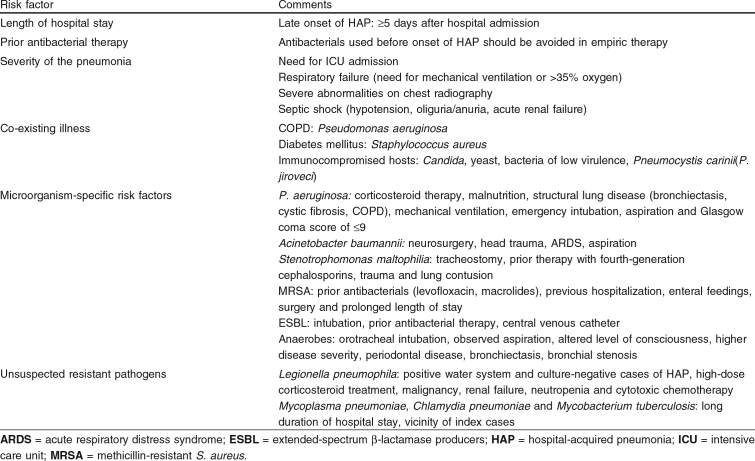
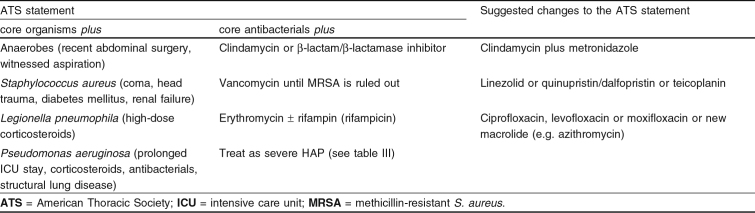
Nosocomial pneumonia or hospital-acquired pneumonia (HAP) causes considerable morbidity and mortality. It is the second most common nosocomial infection and the leading cause of death from hospital-acquired infections. In 1996 the American Thoracic Society (ATS) published guidelines for empirical therapy of HAP. This review focuses on the literature that has appeared since the ATS statement. Early diagnosis of HAP and its etiology is crucial in guiding empirical therapy. Since 1996, it has become clear that differentiating mere colonization from etiologic pathogens infecting the lower respiratory tract is best achieved by employing bronchoalveolar lavage (BAL) or protected specimen brush (PSB) in combination with quantitative culture and detection of intracellular microorganisms. Endotracheal aspirate and non-bronchoscopic BAL/PSB in combination with quantitative culture provide a good alternative in patients suspected of ventilator-associated pneumonia. Since culture results take 2-3 days, initial therapy of HAP is by definition empirical. Epidemiologic studies have identified the most frequently involved pathogens: Enterobacteriaceae, Haemophilus influenzae, Streptococcus pneumoniae and Staphylococcus aureus ('core pathogens'). Empirical therapy covering only the 'core pathogens' will suffice in patients without risk factors for resistant microorganisms. Studies that have appeared since the ATS statement issued in 1996, demonstrate several new risk factors for HAP with multiresistant pathogens. In patients with risk factors, empirical therapy should consist of antibacterials with a broader spectrum. The most important risk factors for resistant microorganisms are late onset of HAP (>/=5 days after admission), recent use of antibacterial therapy, and mechanical ventilation. Multiresistant bacteria of specific interest are methicillin-resistant S. aureus (MRSA), Pseudomonas aeruginosa, Acinetobacter calcoaceticus-baumannii, Stenotrophomonas maltophilia and extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae. Each of these organisms has its specific susceptibility pattern, demanding appropriate antibacterial treatment. To further improve outcomes, specific therapeutic options for multiresistant pathogens and pharmacological factors are discussed. Antibacterials developed since 1996 or antibacterials with renewed interest (linezolid, quinupristin/dalfopristin, teicoplanin, meropenem, new fluoroquinolones, and fourth-generation cephalosporins) are discussed in the light of developing resistance.Since the ATS statement, many reports have shown increasing incidences of resistant microorganisms. Therefore, one of the most important conclusions from this review is that empirical therapy for HAP should not be based on general guidelines alone, but that local epidemiology should be taken into account and used in the formulation of local guidelines.

医院获得性肺炎(HAP)可导致相当高的发病率和死亡率。它是第二常见的医院感染,也是医院获得性感染导致死亡的主要原因。1996年,美国胸科学会(ATS)发布了HAP经验性治疗指南。本综述聚焦于自ATS声明发布以来出现的文献。HAP及其病因的早期诊断对于指导经验性治疗至关重要。自1996年以来,已明确通过采用支气管肺泡灌洗(BAL)或防污染标本刷(PSB)结合定量培养和细胞内微生物检测,能最好地区分单纯定植与感染下呼吸道的病原体。气管内吸出物以及非支气管镜下BAL/PSB结合定量培养为疑似呼吸机相关性肺炎的患者提供了一个很好的替代方法。由于培养结果需要2 - 3天,HAP的初始治疗从定义上讲是经验性的。流行病学研究已确定了最常涉及的病原体:肠杆菌科、流感嗜血杆菌、肺炎链球菌和金黄色葡萄球菌(“核心病原体”)。对于没有耐药微生物危险因素的患者,仅覆盖“核心病原体”的经验性治疗就足够了。自1996年ATS声明发布以来出现的研究表明,HAP合并多重耐药病原体存在几个新的危险因素。对于有危险因素的患者,经验性治疗应包括使用更广谱的抗菌药物。耐药微生物最重要的危险因素是HAP发病较晚(入院后≥5天)、近期使用抗菌治疗以及机械通气。特别值得关注的多重耐药菌包括耐甲氧西林金黄色葡萄球菌(MRSA)、铜绿假单胞菌、鲍曼不动杆菌、嗜麦芽窄食单胞菌以及产超广谱β-内酰胺酶(ESBL)的肠杆菌科细菌。这些微生物各自具有特定的药敏模式,需要进行适当的抗菌治疗。为进一步改善治疗效果,本文讨论了针对多重耐药病原体的具体治疗选择和药理学因素。对1996年以来研发的抗菌药物或重新受到关注的抗菌药物(利奈唑胺、奎奴普丁/达福普汀、替考拉宁、美罗培南、新型氟喹诺酮类药物以及第四代头孢菌素)根据耐药性的发展进行了讨论。自ATS声明发布以来,许多报告显示耐药微生物的发病率不断上升。因此,本综述最重要的结论之一是,HAP的经验性治疗不应仅基于通用指南,而应考虑当地的流行病学情况,并用于制定当地的指南。