Resch Stephen C, Salomon Joshua A, Murray Megan, Weinstein Milton C
Department of Health Policy and Management, Harvard School of Public Health, Harvard University, Boston, Massachusetts, United States of America.
PLoS Med. 2006 Jul;3(7):e241. doi: 10.1371/journal.pmed.0030241.
Despite the existence of effective drug treatments, tuberculosis (TB) causes 2 million deaths annually worldwide. Effective treatment is complicated by multidrug-resistant TB (MDR TB) strains that respond only to second-line drugs. We projected the health benefits and cost-effectiveness of using drug susceptibility testing and second-line drugs in a lower-middle-income setting with high levels of MDR TB.
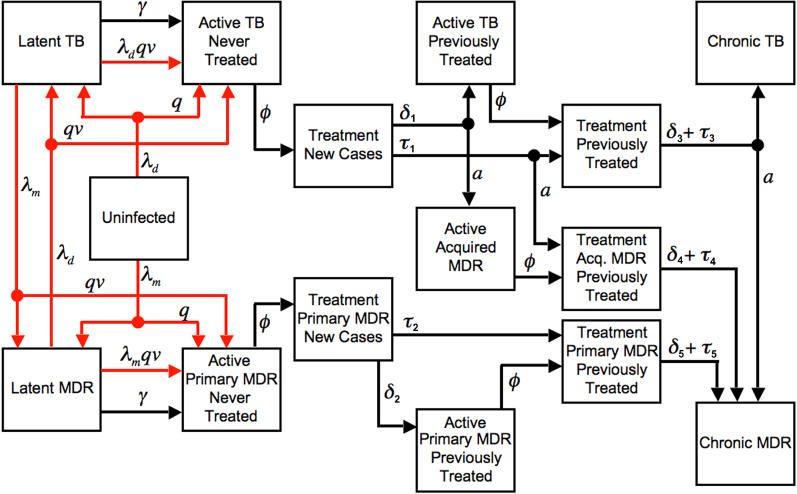
We developed a dynamic state-transition model of TB. In a base case analysis, the model was calibrated to approximate the TB epidemic in Peru, a setting with a smear-positive TB incidence of 120 per 100,000 and 4.5% MDR TB among prevalent cases. Secondary analyses considered other settings. The following strategies were evaluated: first-line drugs administered under directly observed therapy (DOTS), locally standardized second-line drugs for previously treated cases (STR1), locally standardized second-line drugs for previously treated cases with test-confirmed MDR TB (STR2), comprehensive drug susceptibility testing and individualized treatment for previously treated cases (ITR1), and comprehensive drug susceptibility testing and individualized treatment for all cases (ITR2). Outcomes were costs per TB death averted and costs per quality-adjusted life year (QALY) gained. We found that strategies incorporating the use of second-line drug regimens following first-line treatment failure were highly cost-effective compared to strategies using first-line drugs only. In our base case, standardized second-line treatment for confirmed MDR TB cases (STR2) had an incremental cost-effectiveness ratio of 720 dollars per QALY (8,700 dollars per averted death) compared to DOTS. Individualized second-line drug treatment for MDR TB following first-line failure (ITR1) provided more benefit at an incremental cost of 990 dollars per QALY (12,000 dollars per averted death) compared to STR2. A more aggressive version of the individualized treatment strategy (ITR2), in which both new and previously treated cases are tested for MDR TB, had an incremental cost-effectiveness ratio of 11,000 dollars per QALY (160,000 dollars per averted death) compared to ITR1. The STR2 and ITR1 strategies remained cost-effective under a wide range of alternative assumptions about treatment costs, effectiveness, MDR TB prevalence, and transmission.
Treatment of MDR TB using second-line drugs is highly cost-effective in Peru. In other settings, the attractiveness of strategies using second-line drugs will depend on TB incidence, MDR burden, and the available budget, but simulation results suggest that individualized regimens would be cost-effective in a wide range of situations.
尽管存在有效的药物治疗方法,但结核病每年仍在全球导致200万人死亡。有效的治疗因耐多药结核病(MDR-TB)菌株而变得复杂,这些菌株仅对二线药物有反应。我们预计了在耐多药结核病高发的中低收入环境中使用药物敏感性检测和二线药物的健康效益及成本效益。
我们建立了一个结核病动态状态转换模型。在一个基础案例分析中,该模型经过校准以近似秘鲁的结核病疫情,秘鲁涂片阳性结核病发病率为每10万人120例,现患病例中耐多药结核病占4.5%。二次分析考虑了其他环境。评估了以下策略:直接观察治疗(DOTS)下给予一线药物、对既往治疗病例使用当地标准化二线药物(策略1)、对检测确诊为耐多药结核病的既往治疗病例使用当地标准化二线药物(策略2)、对既往治疗病例进行全面药物敏感性检测并个体化治疗(方案1)以及对所有病例进行全面药物敏感性检测并个体化治疗(方案2)。结果指标为避免每例结核病死亡所花费的成本以及每获得一个质量调整生命年(QALY)所花费的成本。我们发现,与仅使用一线药物的策略相比,在一线治疗失败后采用二线药物治疗方案的策略具有很高的成本效益。在我们的基础案例中,与DOTS相比,确诊耐多药结核病病例采用标准化二线治疗(策略2)每QALY的增量成本效益比为720美元(每避免一例死亡8700美元)。一线治疗失败后对耐多药结核病采用个体化二线药物治疗(方案1)与策略2相比,每QALY增量成本为990美元(每避免一例死亡12000美元)时能带来更多益处。一种更积极的个体化治疗策略版本(方案2),即对新发病例和既往治疗病例均进行耐多药结核病检测,与方案1相比,每QALY的增量成本效益比为11000美元(每避免一例死亡160000美元)。在关于治疗成本、有效性、耐多药结核病患病率和传播的一系列替代假设下,策略2和方案1仍然具有成本效益。
在秘鲁,使用二线药物治疗耐多药结核病具有很高的成本效益。在其他环境中,使用二线药物策略的吸引力将取决于结核病发病率、耐多药负担和可用预算,但模拟结果表明,个体化治疗方案在广泛的情况下都具有成本效益。