Merchant Saumil N, Rosowski John J, McKenna Michael J
Department of Otolaryngology, Massachusetts Eye and Ear Infirmary, Boston, Mass., USA.
Adv Otorhinolaryngol. 2007;65:137-145. doi: 10.1159/000098790.
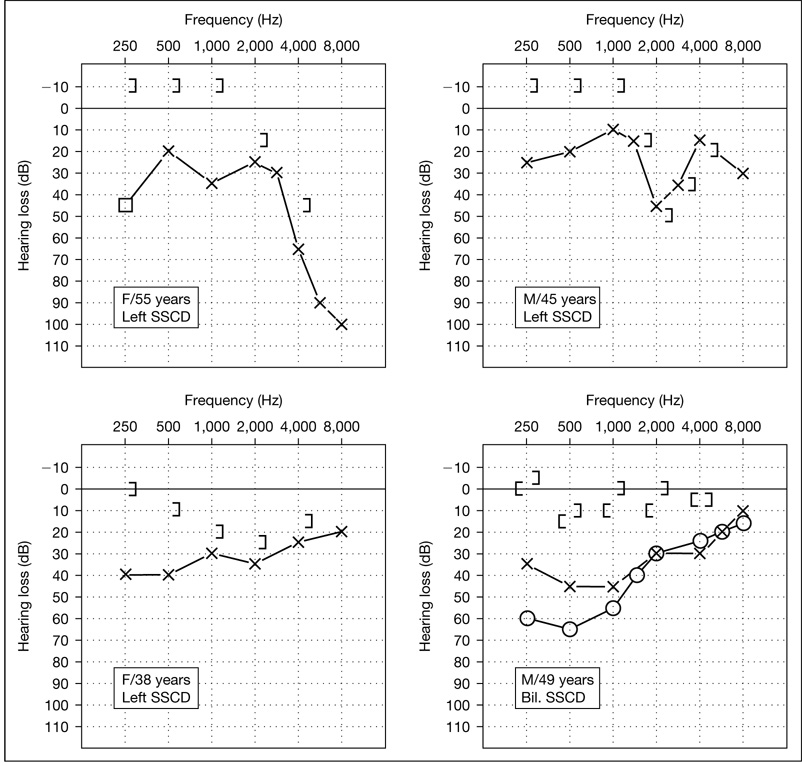
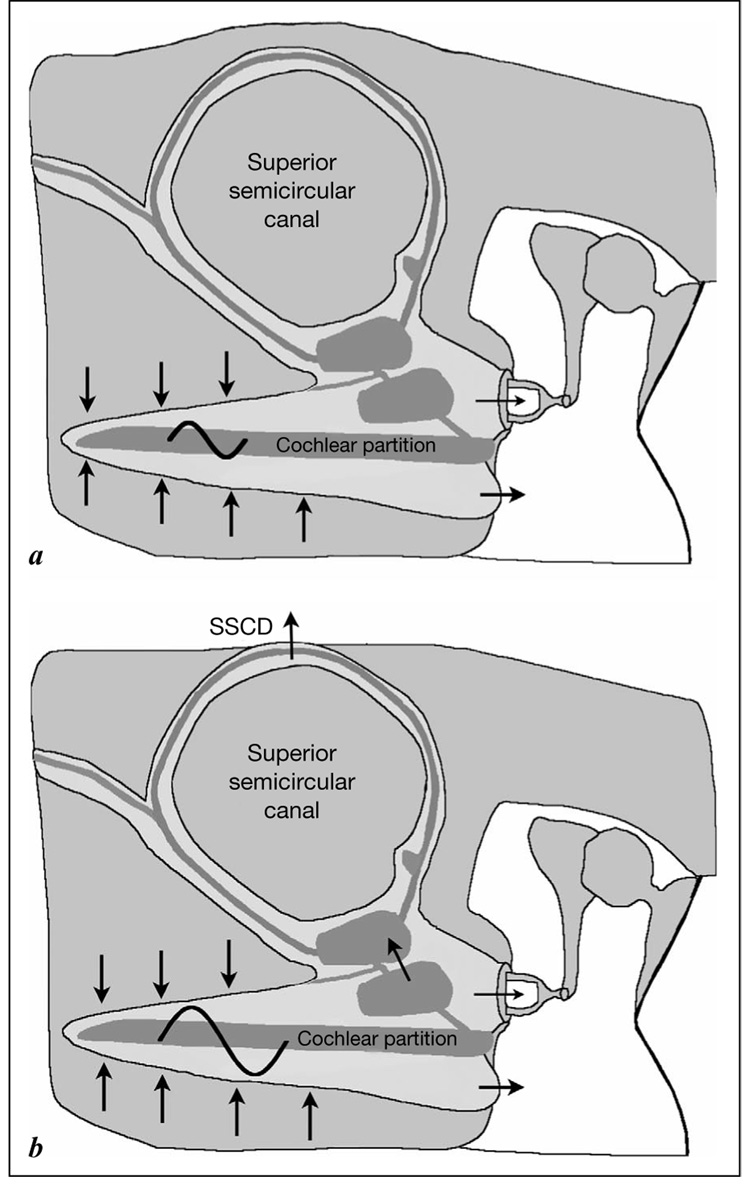
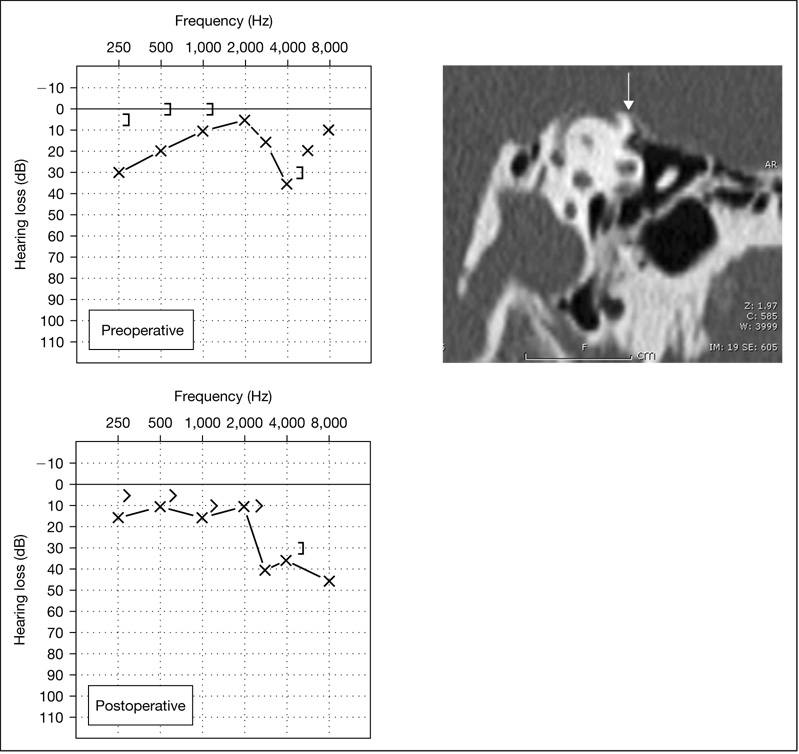
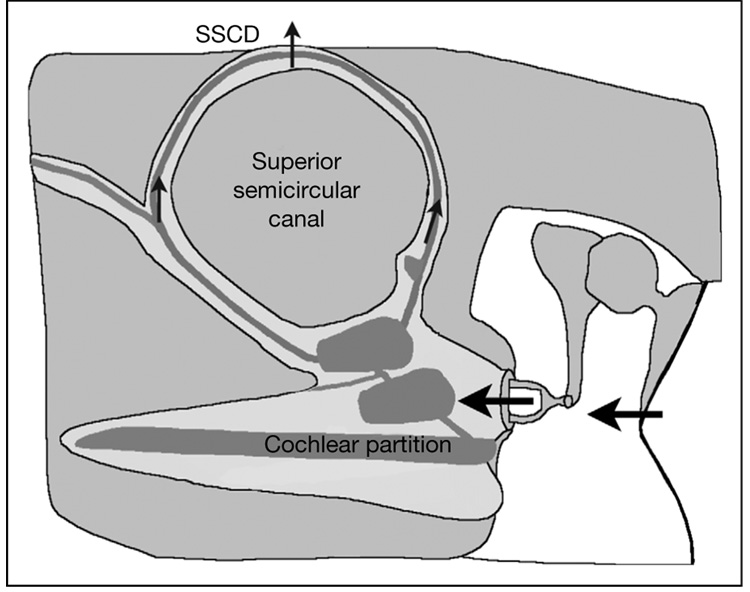
A puzzling aspect of middle ear surgery is the presence of an air-bone gap in a small number of cases with no apparent cause. We believe that some of these cases are due to unrecognized superior semicircular canal dehiscence (SSCD). We have now gathered experience from 20 patients with SSCD presenting with apparent conductive hearing loss without vestibular symptoms. All affected ears had SSCD on high-resolution CT scan. The common findings in these patients were: (1) the air-bone gaps occurred in the lower frequencies below 2,000 Hz, and ranged from 10 to 60 dB; (2) bone conduction thresholds below 2,000 Hz were sometimes negative (-5 dB to -15 dB); (3) the acoustic (stapedial) reflex was present; (4) measurement of umbo velocity by laser Doppler vibrometry showed slight hypermobility of umbo motion; (5) the vestibular-evoked myogenic potential response was present, with thresholds that were abnormally low, and (6) the middle ear was normal at exploratory tympanotomy, including normal mobility of the ossicles and a patent round window niche. We have investigated the mechanism of the air-bone gap due to SSCD using a theoretical framework, clinical research data and an animal model (chinchilla). Our research supports the hypothesis that SSCD introduces a 'third' window into the inner ear which produces the airbone gap by (1) shunting air-conducted sound away from the cochlea, thus elevating air conduction thresholds, and (2) increasing the difference in impedance between the scala tympani and scala vestibuli, thus improving thresholds for bone-conducted sound.
中耳手术中一个令人费解的现象是,在少数病例中存在气骨导差,却没有明显原因。我们认为,其中一些病例是由于未被识别的上半规管裂(SSCD)所致。我们现已积累了20例SSCD患者的经验,这些患者表现为明显的传导性听力损失且无前庭症状。所有患耳在高分辨率CT扫描中均显示有SSCD。这些患者的常见表现为:(1)气骨导差出现在2000Hz以下的低频段,范围为10至60dB;(2)2000Hz以下的骨导阈值有时为负值(-5dB至-15dB);(3)存在声反射(镫骨肌反射);(4)用激光多普勒振动测量法测量鼓膜脐速度显示鼓膜脐运动有轻微的活动过度;(5)存在前庭诱发肌源性电位反应,其阈值异常低;(6)在探查性鼓室切开术中中耳正常,包括听小骨活动正常和圆窗龛通畅。我们利用理论框架、临床研究数据和动物模型(栗鼠)研究了SSCD导致气骨导差的机制。我们的研究支持这样的假说,即SSCD在内耳中引入了一个“第三”窗,通过以下方式产生气骨导差:(1)将气导声音从耳蜗分流,从而提高气导阈值;(2)增加鼓阶和前庭阶之间的阻抗差异,从而改善骨导声音的阈值。