Fartoukh Muriel, Khalil Antoine, Louis Laurence, Carette Marie-France, Bazelly Bernard, Cadranel Jacques, Mayaud Charles, Parrot Antoine
Service de Pneumologie et Unité de Réanimation Respiratoire, Hôpital Tenon, Assistance Publique--Hôpitaux de Paris and Université Pierre et Marie Curie, 4 Rue de la Chine, 75020 Paris, France.
Respir Res. 2007 Feb 15;8(1):11. doi: 10.1186/1465-9921-8-11.
Limited data are available concerning patients admitted to the intensive care unit (ICU) for severe haemoptysis. We reviewed a large series of patients managed in a uniform way to describe the clinical spectrum and outcome of haemoptysis in this setting, and better define the indications for bronchial artery embolisation (BAE).
A retrospective chart review of 196 patients referred for severe haemoptysis to a respiratory intermediate care ward and ICU between January 1999 and December 2001. A follow-up by telephone interview or a visit.
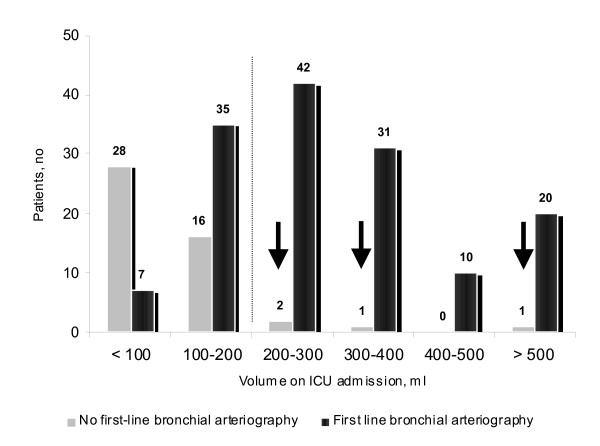
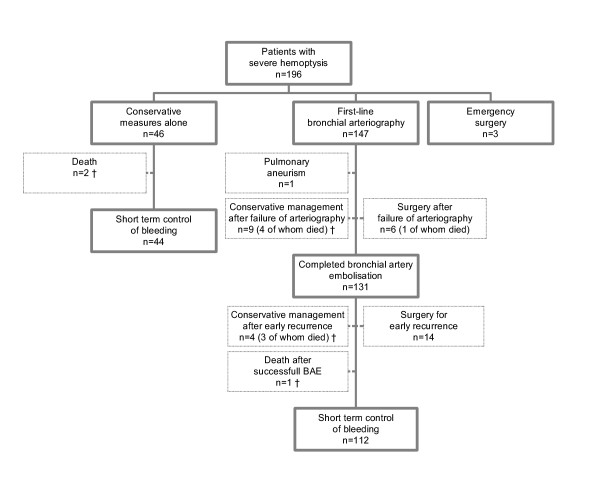
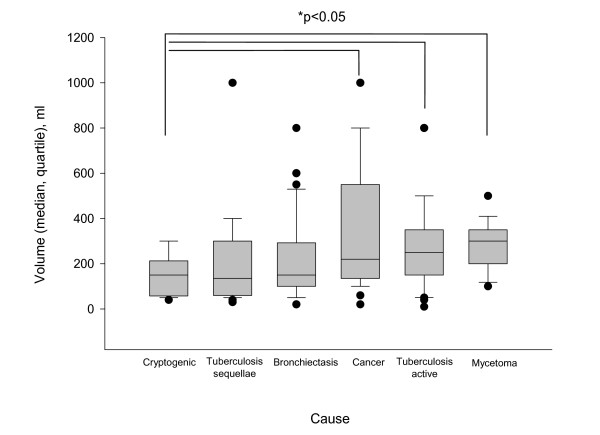
Patients (148 males) were aged 51 (+/- sd, 16) years, with a median cumulated amount of bleeding averaging 200 ml on admission. Bronchiectasis, lung cancer, tuberculosis and mycetoma were the main underlying causes. In 21 patients (11%), no cause was identified. A first-line bronchial arteriography was attempted in 147 patients (75%), whereas 46 (23%) received conservative treatment. Patients who underwent BAE had a higher respiratory rate, greater amount of bleeding, persistent bloody sputum and/or evidence of active bleeding on fiberoptic bronchoscopy. When completed (n = 131/147), BAE controlled haemoptysis in 80% of patients, both in the short and long (> 30 days) terms. Surgery was mostly performed when bronchial arteriography had failed and/or bleeding recurred early after completed BAE. Bleeding was controlled by conservative measures alone in 44 patients. The ICU mortality rate was low (4%).
Patients with evidence of more severe or persistent haemoptysis were more likely to receive BAE rather than conservative management. The procedure was effective and safe in most patients with severe haemoptysis, and surgery was mostly reserved to failure of arteriography and/or early recurrences after BAE.
关于因严重咯血入住重症监护病房(ICU)的患者的数据有限。我们回顾了一大组以统一方式管理的患者,以描述这种情况下咯血的临床谱和结局,并更好地确定支气管动脉栓塞术(BAE)的适应证。
对1999年1月至2001年12月间因严重咯血转诊至呼吸中级护理病房和ICU的196例患者进行回顾性病历审查。通过电话访谈或家访进行随访。
患者(148例男性)年龄为51(±标准差,16)岁,入院时累计出血量中位数平均为200ml。支气管扩张、肺癌、肺结核和肺真菌瘤是主要的潜在病因。21例患者(11%)未查明病因。147例患者(75%)尝试了一线支气管动脉造影,而46例患者(23%)接受了保守治疗。接受BAE的患者呼吸频率更高、出血量更大、持续咯血,和/或纤维支气管镜检查有活动性出血迹象。当完成BAE时(n = 131/147),无论短期还是长期(>30天),80%的患者咯血得到控制。当支气管动脉造影失败和/或BAE完成后早期出血复发时,大多进行手术。44例患者仅通过保守措施控制了出血。ICU死亡率较低(4%)。
有更严重或持续性咯血证据的患者更有可能接受BAE而非保守治疗。该手术对大多数严重咯血患者有效且安全,手术大多保留用于动脉造影失败和/或BAE后早期复发的情况。