Kassaï Behrouz, Boissel Jean-Pierre, Cucherat Michel, Boutitie Florent, Gueyffier François
Department of Clinical Pharmacology, Claude Bernard University, Lyon, France.
Vasc Health Risk Manag. 2005;1(2):163-9. doi: 10.2147/vhrm.1.2.163.64086.
Consideration of absolute risk has been recommended for making decisions concerning preventive treatment in hypertension. We performed simulations to estimate the benefit of antihypertensive therapy over a life-time.
The rate of nonfatal and fatal events of untreated hypertensives in the US population were estimated using data from Individual Data ANalysis of Antihypertensive drug intervention trials (INDANA; a meta-analysis on individual data in hypertension) and specific cause of death from national statistics. Disease-free survival curves until all patients have died were built using the "life-table" method. The treatment effect estimated from INDANA was applied to this curve to obtain the disease-free survival curve of the life-long treated population. Gains in event-free life expectancy (GLE) were estimated from survival curves. A sensitivity analysis was performed to assess the impact of possible death misclassifications.
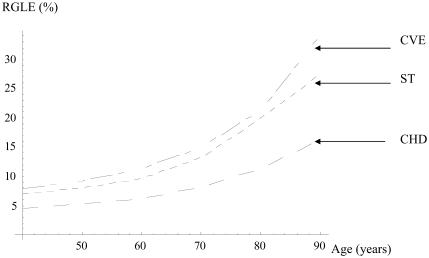
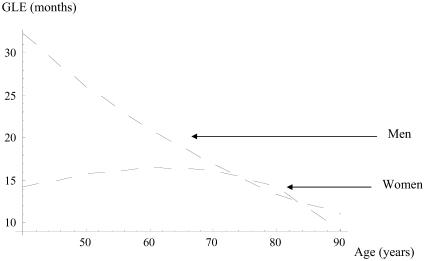
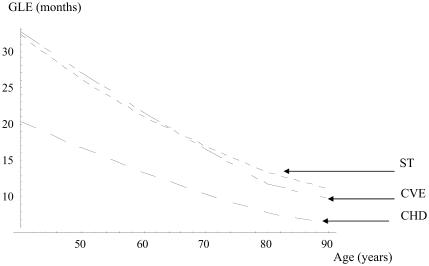
For a 40-year-old man, the gain in life expectancy without stroke and major cardiovascular events were 27 and 32 months, respectively, and were more substantial than those without coronary disease (19 months). The GLE decreased slowly with increasing age at the beginning of treatment, whereas short-term absolute risk reductions increase sharply with age.
Policies based on the selection of patients to treat according to absolute benefit do not maximize the GLE compared with strategies that treat low-risk patients.
在做出高血压预防性治疗决策时,建议考虑绝对风险。我们进行了模拟,以估计终身抗高血压治疗的益处。
利用抗高血压药物干预试验个体数据分析(INDANA;一项关于高血压个体数据的荟萃分析)的数据以及国家统计中的特定死亡原因,估计美国人群中未经治疗的高血压患者的非致命和致命事件发生率。使用“生命表”方法构建直至所有患者死亡的无病生存曲线。将从INDANA估计的治疗效果应用于此曲线,以获得终身接受治疗人群的无病生存曲线。从生存曲线估计无事件预期寿命(GLE)的增加。进行敏感性分析以评估可能的死亡误分类的影响。
对于一名40岁男性,无中风和重大心血管事件的预期寿命增加分别为27个月和32个月,比无冠心病的预期寿命增加(19个月)更为显著。治疗开始时,GLE随着年龄的增加而缓慢下降,而短期绝对风险降低则随着年龄的增长而急剧增加。
与治疗低风险患者的策略相比,基于根据绝对益处选择治疗患者的政策并不能使GLE最大化。