van der Gaag Niels A, de Castro Steve M M, Rauws Erik A J, Bruno Marco J, van Eijck Casper H J, Kuipers Ernst J, Gerritsen Josephus J G M, Rutten Jan-Paul, Greve Jan Willem, Hesselink Erik J, Klinkenbijl Jean H G, Rinkes Inne H M Borel, Boerma Djamila, Bonsing Bert A, van Laarhoven Cees J, Kubben Frank J G M, van der Harst Erwin, Sosef Meindert N, Bosscha Koop, de Hingh Ignace H J T, Th de Wit Laurens, van Delden Otto M, Busch Olivier R C, van Gulik Thomas M, Bossuyt Patrick M M, Gouma Dirk J
Department of Surgery, Academic Medical Center Amsterdam, The Netherlands.
BMC Surg. 2007 Mar 12;7:3. doi: 10.1186/1471-2482-7-3.
Surgery in patients with obstructive jaundice caused by a periampullary (pancreas, papilla, distal bile duct) tumor is associated with a higher risk of postoperative complications than in non-jaundiced patients. Preoperative biliary drainage was introduced in an attempt to improve the general condition and thus reduce postoperative morbidity and mortality. Early studies showed a reduction in morbidity. However, more recently the focus has shifted towards the negative effects of drainage, such as an increase of infectious complications. Whether biliary drainage should always be performed in jaundiced patients remains controversial. The randomized controlled multicenter DROP-trial (DRainage vs. Operation) was conceived to compare the outcome of a 'preoperative biliary drainage strategy' (standard strategy) with that of an 'early-surgery' strategy, with respect to the incidence of severe complications (primary-outcome measure), hospital stay, number of invasive diagnostic tests, costs, and quality of life.
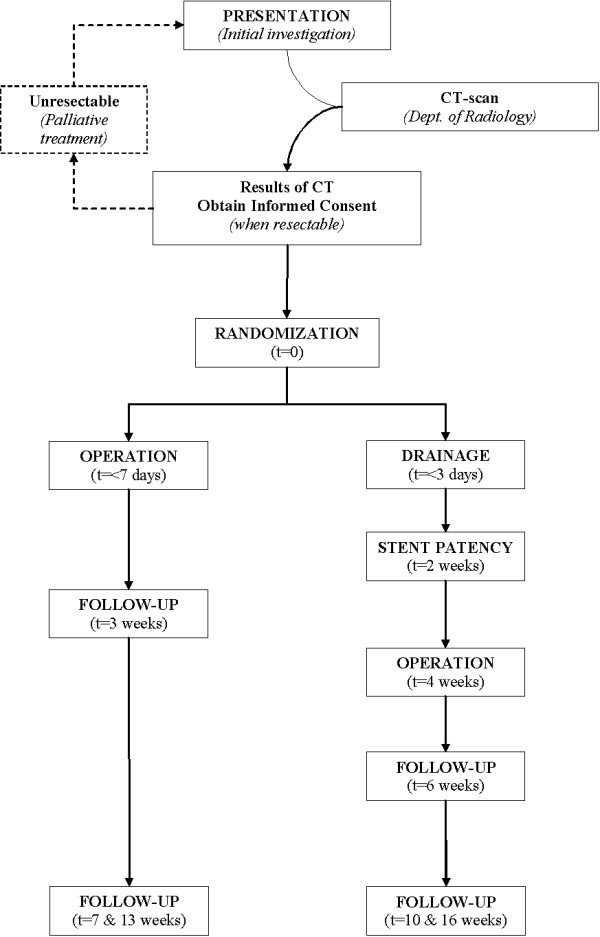
METHODS/DESIGN: Patients with obstructive jaundice due to a periampullary tumor, eligible for exploration after staging with CT scan, and scheduled to undergo a "curative" resection, will be randomized to either "early surgical treatment" (within one week) or "preoperative biliary drainage" (for 4 weeks) and subsequent surgical treatment (standard treatment). Primary outcome measure is the percentage of severe complications up to 90 days after surgery. The sample size calculation is based on the equivalence design for the primary outcome measure. If equivalence is found, the comparison of the secondary outcomes will be essential in selecting the preferred strategy. Based on a 40% complication rate for early surgical treatment and 48% for preoperative drainage, equivalence is taken to be demonstrated if the percentage of severe complications with early surgical treatment is not more than 10% higher compared to standard treatment: preoperative biliary drainage. Accounting for a 10% dropout, 105 patients are needed in each arm resulting in a study population of 210 (alpha = 0.95, beta = 0.8).
The DROP-trial is a randomized controlled multicenter trial that will provide evidence whether or not preoperative biliary drainage is to be performed in patients with obstructive jaundice due to a periampullary tumor.
壶腹周围(胰腺、乳头、远端胆管)肿瘤导致的梗阻性黄疸患者手术,与非黄疸患者相比,术后并发症风险更高。术前胆道引流旨在改善一般状况,从而降低术后发病率和死亡率。早期研究显示发病率有所降低。然而,最近关注点已转向引流的负面影响,如感染性并发症增加。黄疸患者是否应常规进行胆道引流仍存在争议。随机对照多中心DROP试验(引流与手术)旨在比较“术前胆道引流策略”(标准策略)与“早期手术”策略在严重并发症发生率(主要结局指标)、住院时间、侵入性诊断检查次数、费用和生活质量方面的结局。
方法/设计:因壶腹周围肿瘤导致梗阻性黄疸、经CT扫描分期后适合探查且计划进行“根治性”切除的患者,将被随机分为“早期手术治疗”(一周内)或“术前胆道引流”(四周)及随后的手术治疗(标准治疗)。主要结局指标是术后90天内严重并发症的百分比。样本量计算基于主要结局指标的等效性设计。如果发现等效性,比较次要结局对于选择首选策略至关重要。基于早期手术治疗并发症发生率为40%,术前引流为48%,如果早期手术治疗严重并发症百分比与标准治疗:术前胆道引流相比不高于10%,则认为证明了等效性。考虑到10%的失访率,每组需要105例患者,从而得出研究人群为210例(α = 0.95,β = 0.8)。
DROP试验是一项随机对照多中心试验,将为因壶腹周围肿瘤导致梗阻性黄疸的患者是否进行术前胆道引流提供证据。