Gulec Seza A, Mesoloras Geraldine, Dezarn William A, McNeillie Patrick, Kennedy Andrew S
Goshen Cancer Institute, Goshen, IN, USA.
J Transl Med. 2007 Mar 14;5:15. doi: 10.1186/1479-5876-5-15.
Treatment records and follow-up data on 40 patients with primary and metastatic liver malignancies who underwent a single whole-liver treatment with Y-90 resin microspheres (SIR-Spheres Sirtex Medical, Lake Forest, IL) were retrospectively reviewed. The objective of the study was to evaluate the anatomic and physiologic determinants of radiation dose distribution, and the dose response of tumor and liver toxicity in patients with liver malignancies who underwent hepatic arterial Y-90 resin microsphere treatment.
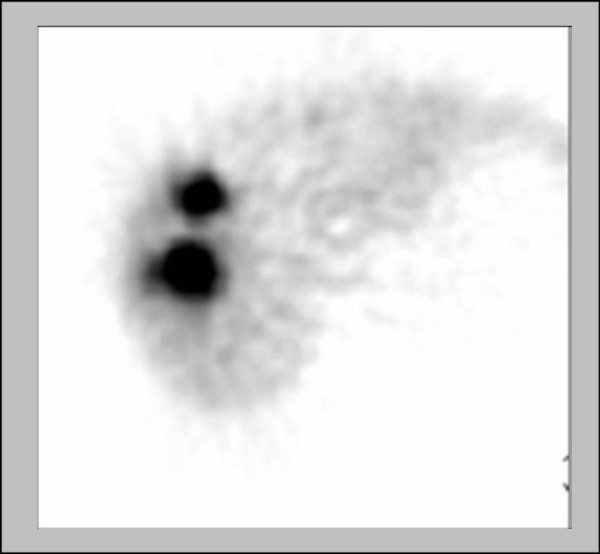
Liver and tumor volume calculations were performed on pre-treatment CT scans. Fractional tumor and liver flow characteristics and lung shunt fractions were determined using hepatic arterial Tc-99m MAA imaging. Absorbed dose calculations were performed using the MIRD equations. Liver toxicity was assessed clinically and by liver function tests. Tumor response to therapy was assessed by CT and/or tumor markers.
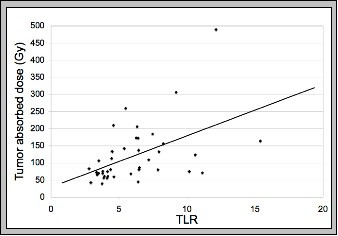
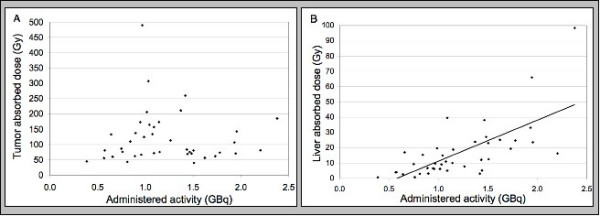
Of the 40 patients, 5 had hepatocellular cancer (HCC), and 35 had metastatic liver tumors (15 colorectal cancer, 10 neuroendocrine tumors, 4 breast cancer, 2 lung cancer, 1 ovarian cancer, 1 endometrial cancer, and 2 unknown primary adenocarcinoma). All patients were treated in a salvage setting with a 3 to 80 week follow-up (mean: 19 weeks). Tumor volumes ranged from 15.0 to 984.2 cc (mean: 294.9 cc) and tumor to normal liver uptake ratios ranged from 2.8 to 15.4 (mean: 5.4). Average administered activity was 1.2 GBq (0.4 to 2.4 GBq). Liver absorbed doses ranged from 0.7 to 99.5 Gy (mean: 17.2 Gy). Tumor absorbed doses ranged from 40.1 to 494.8 Gy (mean: 121.5 Gy). None of the patients had clinical venoocclusive disease or therapy-induced liver failure. Seven patients (17.5 %) had transient and 7 patients (17.5 %) had persistent LFT abnormalities. There were 27 (67.5%) responders (complete response, partial response, and stable disease). Tumor response correlated with higher tumor flow ratio as measured by Tc-99m MAA imaging.
Doses up to 99.5 Gy to uninvolved liver are tolerated with no clinical venoocclusive disease or liver failure. The lowest tumor dose producing a detectable response is 40.1 Gy. The utilization of MAA-based imaging techniques to determine tumor and liver blood flow for clinical treatment planning and the calculation of administered activity may improve clinical outcomes.
回顾性分析了40例原发性和转移性肝恶性肿瘤患者的治疗记录及随访数据,这些患者接受了一次用钇-90树脂微球(SIR-Spheres,Sirtex Medical公司,伊利诺伊州莱克福里斯特)进行的全肝治疗。本研究的目的是评估肝恶性肿瘤患者接受肝动脉钇-90树脂微球治疗时,辐射剂量分布的解剖学和生理学决定因素,以及肿瘤剂量反应和肝毒性。
在治疗前的CT扫描上进行肝脏和肿瘤体积计算。使用肝动脉锝-99m标记的大聚合人血清白蛋白(Tc-99m MAA)显像确定肿瘤和肝脏的血流分数以及肺分流分数。使用医学内照射剂量(MIRD)公式进行吸收剂量计算。通过临床评估和肝功能检查评估肝毒性。通过CT和/或肿瘤标志物评估肿瘤对治疗的反应。
40例患者中,5例为肝细胞癌(HCC),35例为转移性肝肿瘤(15例为结直肠癌,10例为神经内分泌肿瘤,4例为乳腺癌,2例为肺癌,1例为卵巢癌,1例为子宫内膜癌,2例为原发不明腺癌)。所有患者均在挽救性治疗环境中接受治疗,随访时间为3至80周(平均19周)。肿瘤体积范围为15.0至984.2立方厘米(平均294.9立方厘米),肿瘤与正常肝脏摄取比值范围为2.8至15.4(平均5.4)。平均给药活度为1.2吉贝可(0.4至2.4吉贝可)。肝脏吸收剂量范围为0.7至99.5戈瑞(平均17.2戈瑞)。肿瘤吸收剂量范围为40.1至494.8戈瑞(平均121.5戈瑞)。所有患者均未出现临床静脉闭塞性疾病或治疗引起的肝衰竭。7例患者(17.5%)出现短暂性肝功能异常,7例患者(17.5%)出现持续性肝功能异常。有27例(67.5%)患者有反应(完全缓解、部分缓解和病情稳定)。肿瘤反应与通过Tc-99m MAA显像测量的较高肿瘤血流比值相关。
未受累肝脏接受高达99.5戈瑞的剂量时可耐受,无临床静脉闭塞性疾病或肝衰竭。产生可检测反应的最低肿瘤剂量为40.1戈瑞。利用基于MAA的成像技术确定肿瘤和肝脏血流以进行临床治疗计划和计算给药活度可能会改善临床结果。