Sebastian Nikhil T, Tan Yubo, Miller Eric D, Williams Terence M, Alexandra Diaz Dayssy
Department of Radiation Oncology, The Ohio State University Comprehensive Cancer Center - Arthur G. James Cancer Hospital and Richard J. Solove Research Institute, 460 W. 10 Ave, Columbus, OH 43210, USA.
Department of Biomedical Informatics, The Ohio State University College of Medicine, 320 Lincoln Tower, 1800 Cannon Drive, Columbus, OH 43210, USA.
Clin Transl Radiat Oncol. 2019 Jul 26;19:66-71. doi: 10.1016/j.ctro.2019.07.007. eCollection 2019 Nov.
Intrahepatic cholangiocarcinoma (ICC) is a highly lethal malignancy. For patients with locally advanced, unresectable disease, numerous liver-directed therapy options exist, including chemoradiation (CRT), stereotactic body radiation therapy (SBRT), and transarterial radioembolization (TARE). There is no randomized data to inform clinicians regarding the optimal treatment modality.
We used the National Cancer Database (NCDB) to study the overall survival (OS) of patients with ICC treated with CRT, SBRT, and TARE. We used Cox proportional hazards modeling and inverse probability of treatment weighting (IPTW) to account for confounding variables.
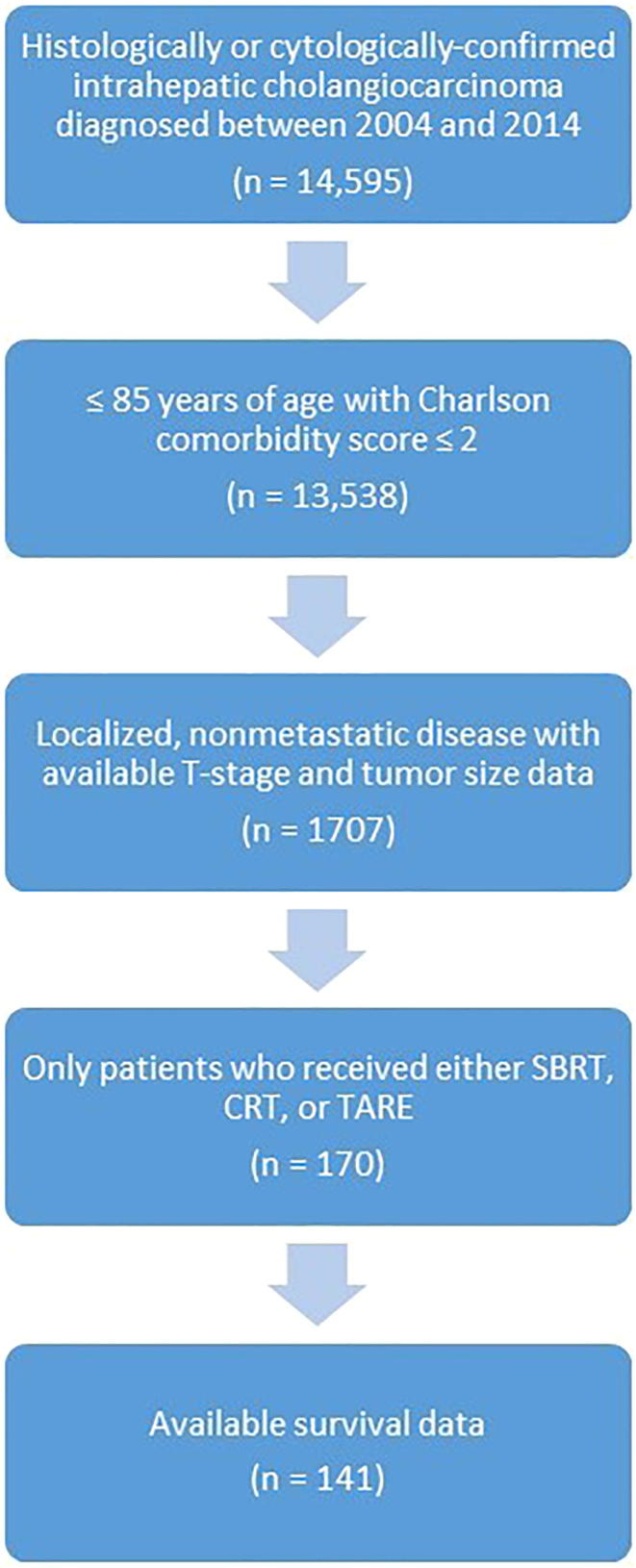
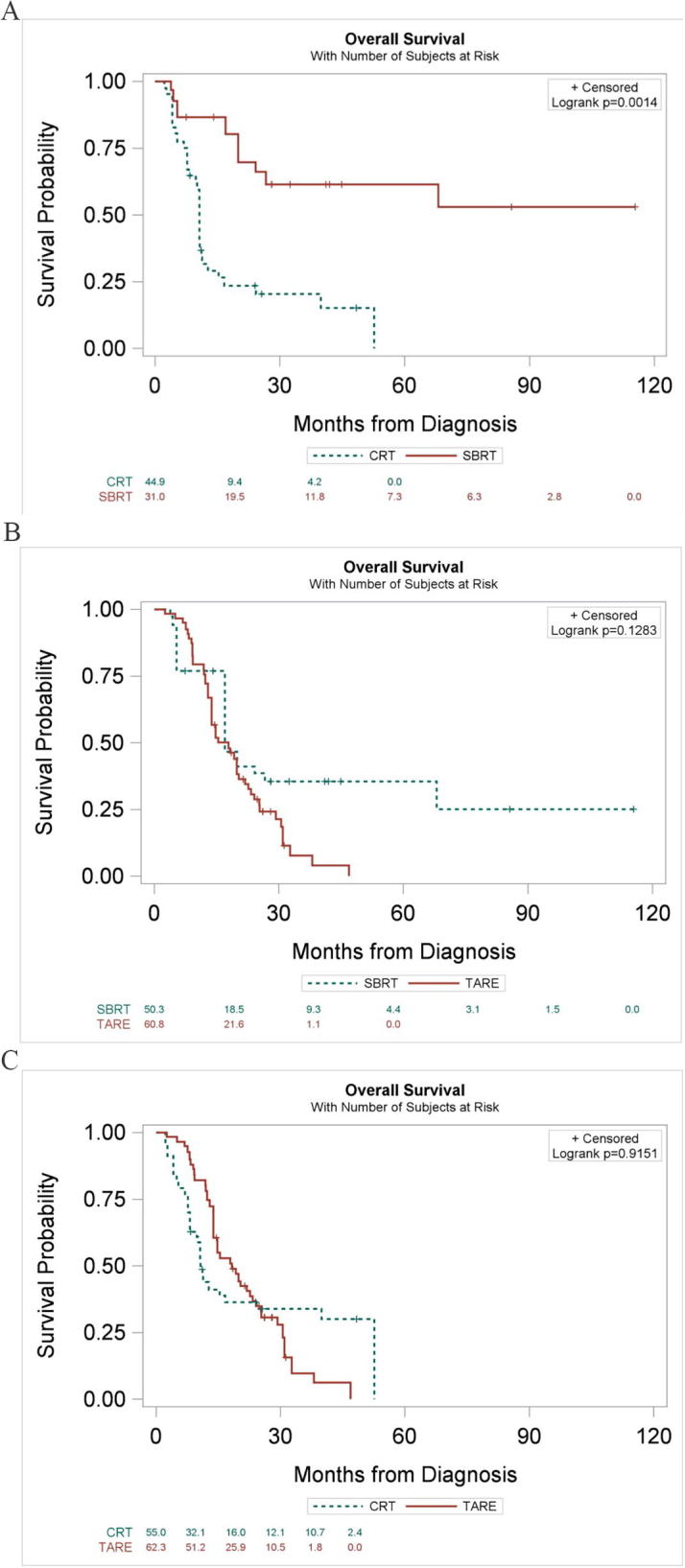
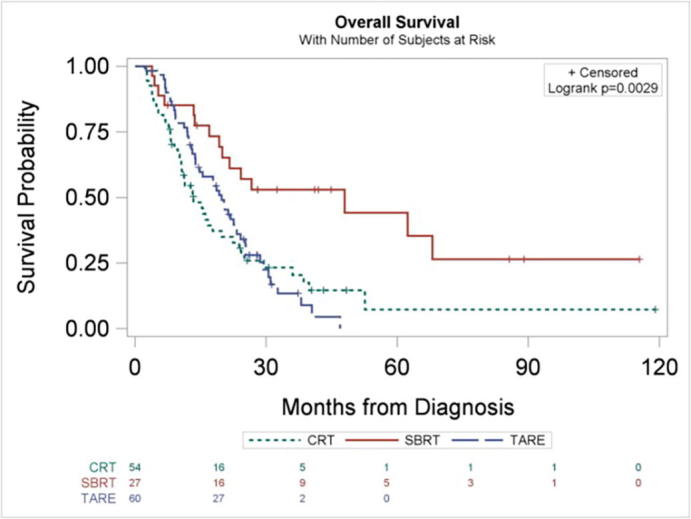
We identified 170 patients with unresected ICC treated with SBRT (n = 37), CRT (n = 61), or TARE (n = 72). SBRT was associated with higher OS compared to CRT (hazard ratio [HR] = 0.37; 95% confidence interval [CI] 0.20-0.68; p = 0.001) and TARE (HR = 0.40; 95% CI 0.22-0.74; p = 0.003). On multivariable analysis, SBRT remained associated with higher OS compared to CRT (HR = 0.44; 95% CI 0.21-0.91; p = 0.028) and TARE (HR = 0.42; 95% CI 0.21-0.84; p = 0.014). After IPTW (Bonferroni-adjusted significance threshold, α = 0.017), SBRT again had a statistically significant association with higher OS compared to CRT (HR = 0.22; 95% CI 0.11-0.44; p < 0.0001) and was nominally associated TARE (HR = 0.58; 95% CI 0.37-0.91; p = 0.019).
We found SBRT is associated with higher OS when compared to CRT or TARE for the treatment of unresectable ICC. Due to the retrospective nature of the study and potential selection bias, these findings should be evaluated prospectively.
肝内胆管癌(ICC)是一种致死率很高的恶性肿瘤。对于局部晚期、无法切除的患者,有多种肝脏定向治疗选择,包括放化疗(CRT)、立体定向体部放射治疗(SBRT)和经动脉放射性栓塞(TARE)。目前尚无随机数据为临床医生提供关于最佳治疗方式的信息。
我们使用国家癌症数据库(NCDB)研究接受CRT、SBRT和TARE治疗的ICC患者的总生存期(OS)。我们使用Cox比例风险模型和治疗权重逆概率(IPTW)来处理混杂变量。
我们确定了170例未切除ICC且接受SBRT(n = 37)、CRT(n = 61)或TARE(n = 72)治疗的患者。与CRT(风险比[HR] = 0.37;95%置信区间[CI] 0.20 - 0.68;p = 0.001)和TARE(HR = 0.40;95% CI 0.22 - 0.74;p = 0.003)相比,SBRT与更高的OS相关。在多变量分析中,与CRT(HR = 0.44;95% CI 0.21 - 0.91;p = 0.028)和TARE(HR = 0.42;95% CI 0.21 - 0.84;p = 0.014)相比,SBRT仍与更高的OS相关。在IPTW后(Bonferroni校正显著性阈值,α = 0.017),与CRT相比,SBRT再次与更高的OS存在统计学显著关联(HR = 0.22;95% CI 0.11 - 0.44;p < 0.0001),并且与TARE存在名义上的关联(HR = 0.58;95% CI 0.37 - 0.91;p = 0.019)。
我们发现,对于无法切除的ICC的治疗,与CRT或TARE相比,SBRT与更高的OS相关。由于本研究的回顾性性质和潜在的选择偏倚,这些发现应进行前瞻性评估。