Kamya Moses R, Yeka Adoke, Bukirwa Hasifa, Lugemwa Myers, Rwakimari John B, Staedke Sarah G, Talisuna Ambrose O, Greenhouse Bryan, Nosten François, Rosenthal Philip J, Wabwire-Mangen Fred, Dorsey Grant
Department of Medicine, Makerere University, Kampala, Uganda.
PLoS Clin Trials. 2007 May 18;2(5):e20. doi: 10.1371/journal.pctr.0020020.
To compare the efficacy and safety of artemether-lumefantrine (AL) and dihydroartemisinin-piperaquine (DP) for treating uncomplicated falciparum malaria in Uganda.
Randomized single-blinded clinical trial.
Apac, Uganda, an area of very high malaria transmission intensity.
Children aged 6 mo to 10 y with uncomplicated falciparum malaria.
Treatment of malaria with AL or DP, each following standard 3-d dosing regimens.
Risks of recurrent parasitemia at 28 and 42 d, unadjusted and adjusted by genotyping to distinguish recrudescences and new infections.
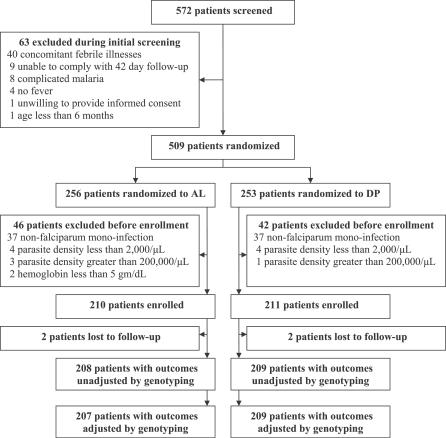
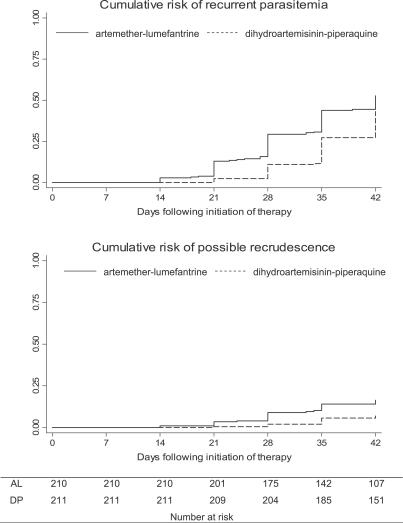
Of 421 enrolled participants, 417 (99%) completed follow-up. The unadjusted risk of recurrent falciparum parasitemia was significantly lower for participants treated with DP than for those treated with AL after 28 d (11% versus 29%; risk difference [RD] 18%, 95% confidence interval [CI] 11%-26%) and 42 d (43% versus 53%; RD 9.6%, 95% CI 0%-19%) of follow-up. Similarly, the risk of recurrent parasitemia due to possible recrudescence (adjusted by genotyping) was significantly lower for participants treated with DP than for those treated with AL after 28 d (1.9% versus 8.9%; RD 7.0%, 95% CI 2.5%-12%) and 42 d (6.9% versus 16%; RD 9.5%, 95% CI 2.8%-16%). Patients treated with DP had a lower risk of recurrent parasitemia due to non-falciparum species, development of gametocytemia, and higher mean increase in hemoglobin compared to patients treated with AL. Both drugs were well tolerated; serious adverse events were uncommon and unrelated to study drugs.
DP was superior to AL for reducing the risk of recurrent parasitemia and gametocytemia, and provided improved hemoglobin recovery. DP thus appears to be a good alternative to AL as first-line treatment of uncomplicated malaria in Uganda. To maximize the benefit of artemisinin-based combination therapy in Africa, treatment should be integrated with aggressive strategies to reduce malaria transmission intensity.
比较蒿甲醚-本芴醇(AL)和双氢青蒿素-哌喹(DP)治疗乌干达非复杂性恶性疟的疗效与安全性。
随机单盲临床试验。
乌干达阿帕克,一个疟疾传播强度非常高的地区。
6个月至10岁患有非复杂性恶性疟的儿童。
用AL或DP治疗疟疾,均采用标准的3天给药方案。
28天和42天时复发性寄生虫血症的风险,通过基因分型进行未调整及调整以区分再燃和新感染。
421名登记参与者中,417名(99%)完成随访。随访28天(11%对29%;风险差[RD]18%,95%置信区间[CI]11%-26%)和42天(43%对53%;RD 9.6%,95%CI 0%-19%)后,接受DP治疗的参与者非复杂性恶性疟复发性寄生虫血症的未调整风险显著低于接受AL治疗的参与者。同样,因可能再燃(经基因分型调整)导致的复发性寄生虫血症风险,在随访28天(1.9%对8.9%;RD 7.0%,95%CI 2.5%-12%)和42天(6.9%对16%;RD 9.5%,95%CI 2.8%-16%)时,接受DP治疗的参与者也显著低于接受AL治疗的参与者。与接受AL治疗的患者相比,接受DP治疗的患者因非恶性疟原虫种类导致的复发性寄生虫血症风险更低,配子体血症发生率更低,血红蛋白平均升高幅度更大。两种药物耐受性均良好;严重不良事件罕见且与研究药物无关。
在降低复发性寄生虫血症和配子体血症风险以及改善血红蛋白恢复方面,DP优于AL。因此,在乌干达,DP似乎是作为非复杂性疟疾一线治疗药物替代AL的良好选择。为使非洲基于青蒿素的联合疗法效益最大化,治疗应与积极降低疟疾传播强度的策略相结合。