Groeneveld A B Johan
Department of Intensive Care, Institute for Cardiovascular Research, Vrije Universiteit Medical Center, Amsterdam, The Netherlands.
BMC Anesthesiol. 2007 Jul 9;7:7. doi: 10.1186/1471-2253-7-7.
Trauma and surgery may be complicated by pulmonary dysfunction, acute lung injury (ALI) and acute respiratory distress syndrome (ARDS), but the mechanisms are incompletely understood.
We evaluated lung capillary protein permeability non-invasively with help of the 67Ga-transferrin pulmonary leak index (PLI) technique and extravascular lung water (EVLW) by the transpulmonary thermal-dye dilution technique in consecutive, mechanically ventilated patients in the intensive care unit within 24 h of direct, blunt thoracic trauma (n = 5, 2 with ARDS), and within 12 h of indirect trauma by transhiatal oesophagectomy (n = 8), abdominal surgery for cancer (n = 6) and bone surgery (n = 4). We studied transfusion history, haemodynamics, oxygenation and mechanics of the lungs. The lung injury score (LIS, 0-4) was calculated. Plain radiography was also done to judge densities and atelectasis.
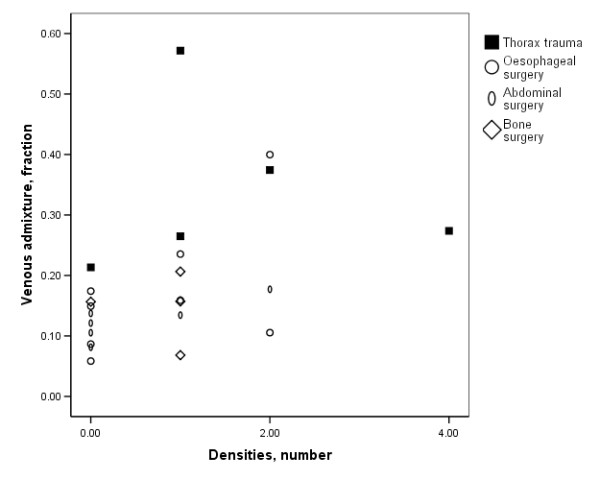
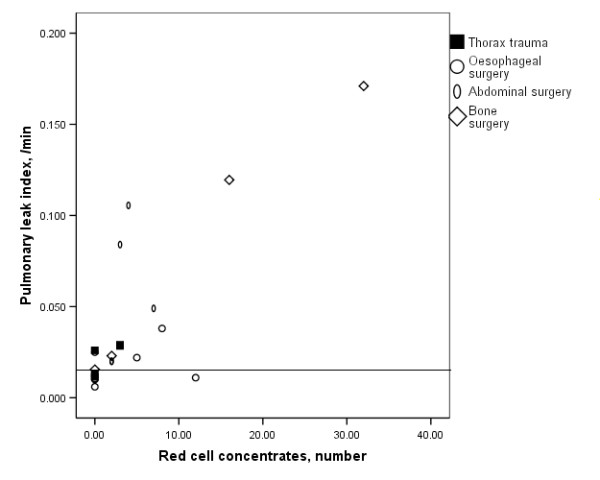
The PLI and EVLW were elevated above normal in 61 and 30% of patients, respectively, and the PLI directly related to the number of red cell concentrates given (rs = 0.69, P < 0.001), without group differences. Oxygenation, lung mechanics, radiographic densities and thus the LIS (1.0 [0.25-3.5]) did not relate to PLI and EVLW. However, groups differed in oxygenation and airway pressures and impaired oxygenation related to the number of radiographic quadrants with densities (rs = 0.55, P = 0.007). Thoracic trauma patients had a worse oxygenation requiring higher airway pressures and thus higher LIS than the other patient groups, unrelated to PLI and EVLW but attributable to a higher cardiac output and thereby venous admixture. Finally, patients with radiographic signs of atelectasis had more impaired oxygenation and more densities than those without.
The oxygenation defect and radiographic densities in mechanically ventilated patients with pulmonary dysfunction and ALI/ARDS after trauma and surgery are likely caused by atelectasis rather than by increased permeability-oedema related to red cell transfusion.
创伤和手术可能并发肺功能障碍、急性肺损伤(ALI)和急性呼吸窘迫综合征(ARDS),但其机制尚未完全明确。
我们采用67Ga-转铁蛋白肺渗漏指数(PLI)技术无创评估肺毛细血管蛋白通透性,并通过经肺热染料稀释技术测量血管外肺水(EVLW)。研究对象为重症监护病房内连续的机械通气患者,其中直接钝性胸部创伤患者于创伤后24小时内纳入(n = 5,2例患有ARDS),经裂孔食管切除术间接创伤患者于创伤后12小时内纳入(n = 8),癌症腹部手术患者(n = 6)和骨手术患者(n = 4)。我们研究了输血史、血流动力学、氧合情况及肺力学。计算肺损伤评分(LIS,0 - 4分)。同时进行胸部X线平片检查以判断肺部密度和肺不张情况。
分别有61%和30%的患者PLI和EVLW高于正常水平,PLI与输注红细胞悬液的数量直接相关(rs = 0.69,P < 0.001),且无组间差异。氧合情况、肺力学、影像学密度以及LIS(1.0 [0.25 - 3.5])与PLI和EVLW无关。然而,不同组间氧合情况和气道压力存在差异,氧合受损与出现肺部密度影的象限数量相关(rs = 0.55,P = 0.007)。胸部创伤患者的氧合情况较差,需要更高的气道压力,因此LIS高于其他患者组,这与PLI和EVLW无关,而是归因于较高的心输出量及由此导致的静脉血掺杂。最后,有肺不张影像学表现的患者比无此表现的患者氧合受损更严重,肺部密度影更多。
创伤和手术后发生肺功能障碍及ALI/ARDS的机械通气患者出现的氧合缺陷和影像学密度改变,可能是由肺不张引起,而非与红细胞输血相关的通透性水肿增加所致。