Hofhuis José G M, Spronk Peter E, van Stel Henk F, Schrijvers Augustinus J P, Bakker Jan
Department of Intensive Care Medicine, Gelre Hospitals (location Lukas), Albert Schweitzerlaan, 7334 DZ Apeldoorn, The Netherlands.
Crit Care. 2007;11(4):R78. doi: 10.1186/cc5970.
Predicting whether a critically ill patient will survive intensive care treatment remains difficult. The advantages of a validated strategy to identify those patients who will not benefit from intensive care unit (ICU) treatment are evident. Providing critical care treatment to patients who will ultimately die in the ICU is accompanied by an enormous emotional and physical burden for both patients and their relatives. The purpose of the present study was to examine whether health-related quality of life (HRQOL) before admission to the ICU can be used as a predictor of mortality.
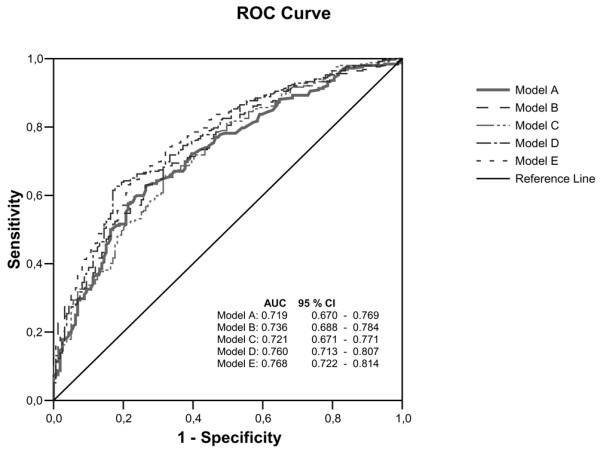
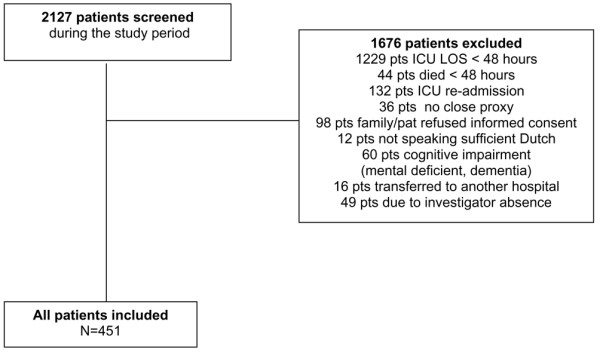
We conducted a prospective cohort study in a university-affiliated teaching hospital. Patients admitted to the ICU for longer than 48 hours were included. Close relatives completed the Short-form 36 (SF-36) within the first 48 hours of admission to assess pre-admission HRQOL of the patient. Mortality was evaluated from ICU admittance until 6 months after ICU discharge. Logistic regression and receiver operating characteristic analyses were used to assess the predictive value for mortality using five models: the first question of the SF-36 on general health (model A); HRQOL measured using the physical component score (PCS) and mental component score (MCS) of the SF-36 (model B); the Acute Physiology and Chronic Health Evaluation (APACHE) II score (an accepted mortality prediction model in ICU patients; model C); general health and APACHE II score (model D); and PCS, MCS and APACHE II score (model E). Classification tables were used to assess the sensitivity, specificity, positive and negative predictive values, and likelihood ratios.
A total of 451 patients were included within 48 hours of admission to the ICU. At 6 months of follow up, 159 patients had died and 40 patients were lost to follow up. When the general health item was used as an estimate of HRQOL, area under the curve for model A (0.719) was comparable to that of model C (0.721) and slightly better than that of model D (0.760). When PCS and MCS were used, the area under the curve for model B (0.736) was comparable to that of model C (0.721) and slightly better than that of model E (0.768). When using the general health item, the sensitivity and specificity in model D (sensitivity 0.52 and specificity 0.81) were similar to those in model A (0.45 and 0.80). Similar results were found when using the MCS and PCS.
This study shows that the pre-admission HRQOL measured with either the one-item general health question or the complete SF-36 is as good at predicting survival/mortality in ICU patients as the APACHE II score. The value of these measures in clinical practice is limited, although it seems sensible to incorporate assessment of HRQOL into the many variables considered when deciding whether a patient should be admitted to the ICU.
预测危重症患者能否在重症监护治疗中存活仍然困难重重。采用经过验证的策略来识别那些无法从重症监护病房(ICU)治疗中获益的患者,其优势显而易见。为最终会在ICU死亡的患者提供重症监护治疗,会给患者及其亲属带来巨大的情感和身体负担。本研究的目的是检验ICU入院前的健康相关生活质量(HRQOL)是否可作为死亡率的预测指标。
我们在一家大学附属医院开展了一项前瞻性队列研究。纳入在ICU住院超过48小时的患者。近亲在入院后的头48小时内完成36项简短健康调查问卷(SF-36),以评估患者入院前的HRQOL。从ICU入院直至出院后6个月评估死亡率。采用逻辑回归和受试者工作特征分析,使用五个模型评估死亡率的预测价值:SF-36关于总体健康的第一个问题(模型A);使用SF-36的身体成分评分(PCS)和心理成分评分(MCS)测量的HRQOL(模型B);急性生理与慢性健康状况评估(APACHE)II评分(ICU患者公认的死亡率预测模型;模型C);总体健康和APACHE II评分(模型D);以及PCS、MCS和APACHE II评分(模型E)。使用分类表评估敏感性、特异性、阳性和阴性预测值以及似然比。
共有451名患者在入住ICU的48小时内被纳入研究。在6个月的随访中,159名患者死亡,40名患者失访。当将总体健康项目用作HRQOL的评估指标时,模型A的曲线下面积(0.719)与模型C(0.721)相当,略优于模型D(0.760)。当使用PCS和MCS时,模型B的曲线下面积(0.736)与模型C(0.721)相当,略优于模型E(0.768)。当使用总体健康项目时,模型D的敏感性和特异性(敏感性0.52,特异性0.81)与模型A(0.45和0.80)相似。使用MCS和PCS时也发现了类似结果。
本研究表明,用单项总体健康问题或完整的SF-36测量的入院前HRQOL在预测ICU患者的生存/死亡率方面与APACHE II评分一样有效。这些指标在临床实践中的价值有限,尽管在决定患者是否应入住ICU时,将HRQOL评估纳入众多考虑变量中似乎是合理的。