Gutiérrez Alonso N, Westerly David C, Tomé Wolfgang A, Jaradat Hazim A, Mackie Thomas R, Bentzen Søren M, Khuntia Deepak, Mehta Minesh P
Department of Medical Physics, University of Wisconsin School of Medicine and Public Health, Madison, WI 53792, USA.
Int J Radiat Oncol Biol Phys. 2007 Oct 1;69(2):589-97. doi: 10.1016/j.ijrobp.2007.05.038.
To evaluate the feasibility of using tomotherapy to deliver whole brain radiotherapy with hippocampal avoidance, hypothesized to reduce the risk of memory function decline, and simultaneously integrated boost to brain metastases to improve intracranial tumor control.
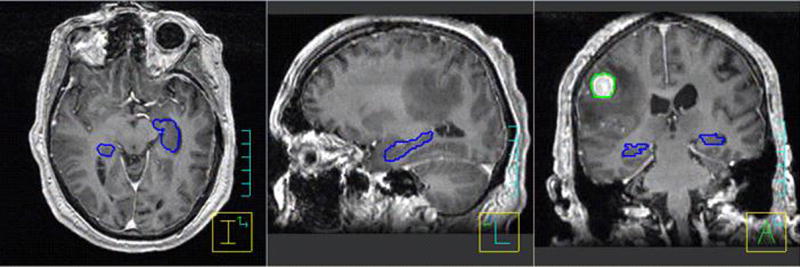
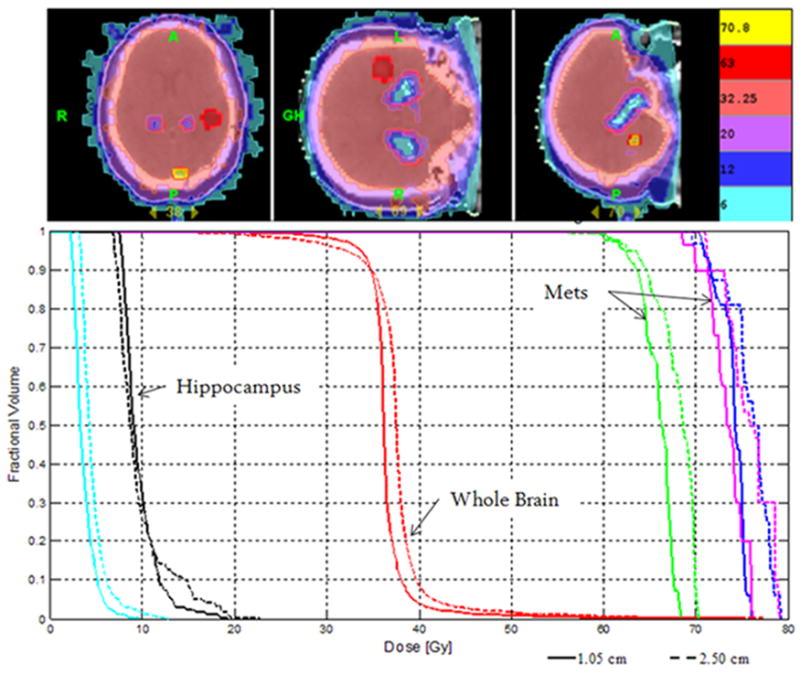
Ten patients treated with radiosurgery and whole brain radiotherapy underwent repeat planning using tomotherapy with the original computed tomography scans and magnetic resonance imaging-computed tomography fusion-defined target and normal structure contours. The individually contoured hippocampus was used as a dose-limiting structure (<6 Gy); the whole brain dose was prescribed at 32.25 Gy to 95% in 15 fractions, and the simultaneous boost doses to individual brain metastases were 63 Gy to lesions >or=2.0 cm in the maximal diameter and 70.8 Gy to lesions <2.0 cm. The plans were generated with a field width (FW) of 2.5 cm and, in 5 patients, with a FW of 1.0 cm. The plans were compared regarding conformation number, prescription isodose/target volume ratio, target coverage, homogeneity index, and mean normalized total dose.
A 1.0-cm FW compared with a 2.5-cm FW significantly improved the dose distribution. The mean conformation number improved from 0.55 +/- 0.16 to 0.60 +/- 0.13. Whole brain homogeneity improved by 32% (p <0.001). The mean normalized total dose to the hippocampus was 5.9 +/- 1.3 Gy(2) and 5.8 +/- 1.9 Gy(2) for 2.5- and 1.0-cm FW, respectively. The mean treatment delivery time for the 2.5- and 1.0-cm FW plans was 10.2 +/- 1.0 and 21.8 +/- 1.8 min, respectively.
Composite tomotherapy plans achieved three objectives: homogeneous whole brain dose distribution equivalent to conventional whole brain radiotherapy; conformal hippocampal avoidance; and radiosurgically equivalent dose distributions to individual metastases.
评估使用断层放疗进行全脑放疗并避开海马体的可行性,据推测这可降低记忆功能衰退的风险,同时对脑转移瘤进行同步推量放疗以改善颅内肿瘤控制。
10例接受过放射外科手术和全脑放疗的患者使用断层放疗进行重复计划,采用原始计算机断层扫描以及磁共振成像 - 计算机断层扫描融合定义的靶区和正常结构轮廓。将个体化勾勒出的海马体用作剂量限制结构(<6 Gy);全脑剂量规定为32.25 Gy,分15次给予95%的体积,对单个脑转移瘤的同步推量剂量对于最大直径≥2.0 cm的病灶为63 Gy,对于直径<2.0 cm的病灶为70.8 Gy。计划生成时的射野宽度(FW)为2.5 cm,5例患者的射野宽度为1.0 cm。对计划在适形数、处方等剂量线/靶区体积比、靶区覆盖、均匀性指数和平均归一化总剂量方面进行比较。
与2.5 cm的射野宽度相比,1.0 cm的射野宽度显著改善了剂量分布。平均适形数从0.55±0.16提高到0.60±0.13。全脑均匀性提高了32%(p<0.001)。对于2.5 cm和1.0 cm射野宽度,海马体的平均归一化总剂量分别为5.9±1.3 Gy(2)和5.8±1.9 Gy(2)。2.5 cm和1.0 cm射野宽度计划的平均治疗实施时间分别为10.2±1.0分钟和21.8±1.8分钟。
复合断层放疗计划实现了三个目标:与传统全脑放疗等效的均匀全脑剂量分布;适形的海马体避让;以及与放射外科手术等效的单个转移瘤剂量分布。