Asmar Roland, Garcia-Puig Juan, Gosse Philippe, Karpov Yuri A, De Leeuws Peter Wilhem, Magometschniggs Dieter, Matos Lajos, Schmieder Roland
Institut Cardiovasculaire, Paris, France.
Vasc Health Risk Manag. 2007;3(4):371-80.
Ambulatory blood pressure (BP) is more sensitive than office BP and is highly correlated with the left ventricular mass (LVM) of hypertensive patients with left ventricular hypertrophy (LVH).
In this prospectively designed ancillary study of the PICXEL trial, the effects of first-line combination perindopril/indapamide on ambulatory BP were compared with those of monotherapy with enalapril in 127 patients. Hypertensive patients with LVH received once daily either perindopril 2 mg/indapamide 0.625 mg (n = 65) or enalapril 10 mg (n = 62) for 52 weeks. Dose adjustments were allowed for uncontrolled BP. Twenty-four-hour ambulatory BP and echocardiographic parameters were measured at baseline, week 24, and week 52.
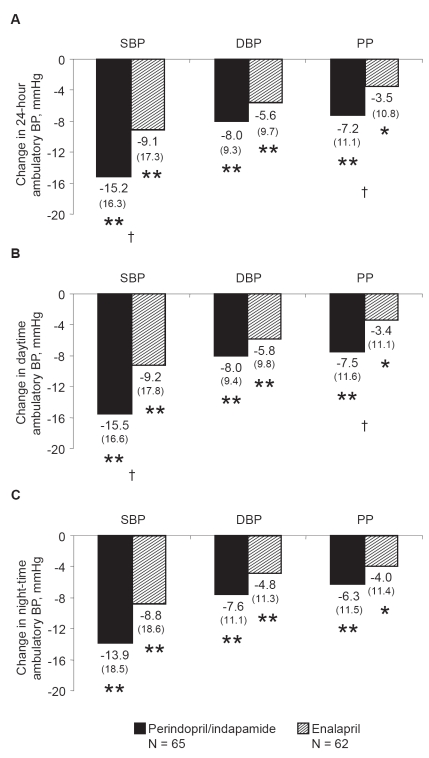
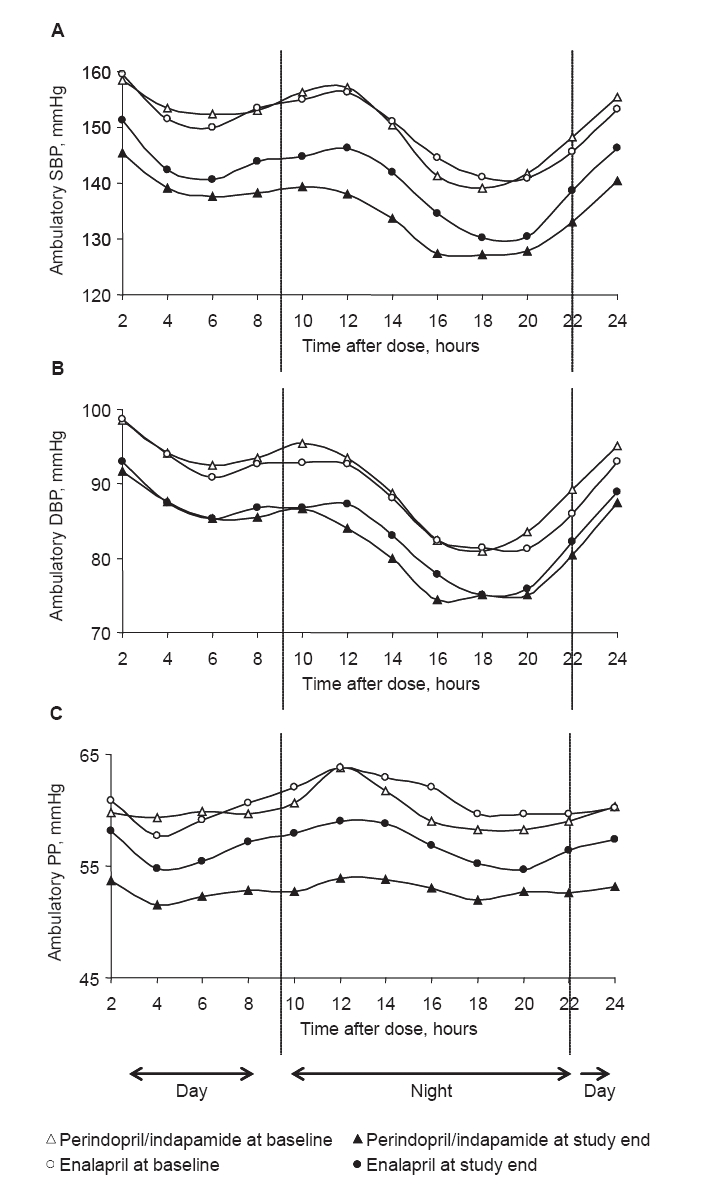
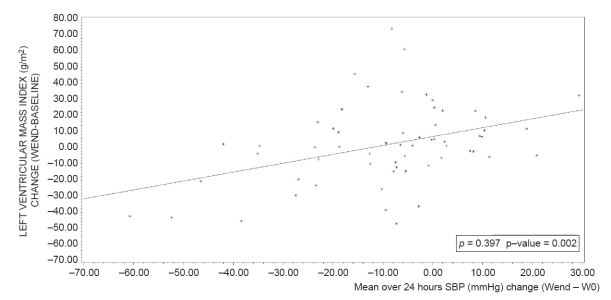
At study end, both treatments significantly improved ambulatory BP compared with baseline (p < or = 0.01). Perindopril/indapamide treatment reduced 24-hour and daytime systolic BP (SBP) and pulse pressure (PP) significantly more than enalapril treatment (p < 0.01). No significant between-group differences were noted for diastolic BP (DBP) or for night-time measurements. Trough/peak ratios were higher with perindopril/indapamide than with enalapril (88.5 vs 65.8 for SBP and 86.7 vs 63.9 for DBP, respectively). The global smoothness index was higher with perindopril/indapamide than with enalapril (6.6 vs 5.2 for SBP and 5.6 vs 4.9 for DBP, respectively). With perindopril/indapamide treatment, LVM index was significantly reduced (-9.1 g/m2 from baseline; p vs baseline <0.001). More patients required dose increases with enalapril (87%) than with perindopril/indapamide (71%). No unusual safety elements were noted.
First-line perindopril/indapamide combination decreased ambulatory SBP and PP, and LVM more effectively than enalapril.
动态血压比诊室血压更敏感,且与左心室肥厚(LVH)的高血压患者的左心室质量(LVM)高度相关。
在这项前瞻性设计的PICXEL试验的辅助研究中,将127例患者一线联合使用培哚普利/吲达帕胺与依那普利单药治疗对动态血压的影响进行了比较。患有LVH的高血压患者每天服用一次培哚普利2mg/吲达帕胺0.625mg(n = 65)或依那普利10mg(n = 62),持续52周。对于血压控制不佳者允许调整剂量。在基线、第24周和第52周测量24小时动态血压和超声心动图参数。
在研究结束时,与基线相比,两种治疗均显著改善了动态血压(p≤0.01)。培哚普利/吲达帕胺治疗比依那普利治疗更显著地降低了24小时和日间收缩压(SBP)及脉压(PP)(p < 0.01)。舒张压(DBP)或夜间测量值在组间无显著差异。培哚普利/吲达帕胺的谷峰比高于依那普利(SBP分别为88.5对65.8,DBP分别为86.7对63.9)。培哚普利/吲达帕胺的整体平滑指数高于依那普利(SBP分别为6.6对5.2,DBP分别为5.6对4.9)。接受培哚普利/吲达帕胺治疗时,LVM指数显著降低(较基线降低9.1g/m²;与基线相比p < 0.001)。与培哚普利/吲达帕胺(71%)相比,更多依那普利治疗的患者需要增加剂量(87%)。未发现异常安全问题。
一线培哚普利/吲达帕胺联合治疗比依那普利更有效地降低了动态SBP和PP以及LVM。