Olson Lyle J, Arruda-Olson Adelaide M, Somers Virend K, Scott Christopher G, Johnson Bruce D
Division of Cardiovascular Diseases, Mayo Clinic College of Medicine, 200 First St SW, Rochester, MN 55905, USA.
Chest. 2008 Feb;133(2):474-81. doi: 10.1378/chest.07-2146. Epub 2007 Dec 10.
Instability of breathing control due to heart failure (HF) manifests as exercise oscillatory ventilation (EOV). Prior descriptions of patients with EOV have not been controlled and have been limited to subjects with left ventricular ejection fraction (LVEF) of <or= 0.40. The aim of this study was to compare clinical characteristics including ventilatory responses of subjects with EOV to those of control subjects with HF matched for LVEF.
Subjects (n = 47) were retrospectively identified from 1,340 consecutive patients referred for cardiopulmonary exercise testing. Study inclusion required EOV without consideration of LVEF while control subjects (n = 47) were composed of HF patients with no EOV matched for LVEF. Characteristics for each group were summarized and compared.
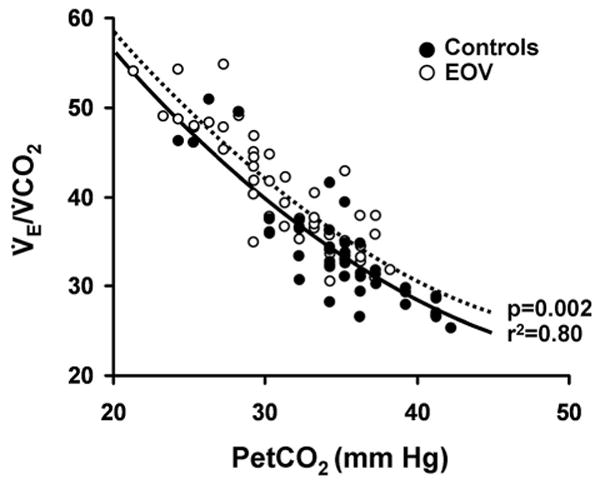
For EOV subjects, the mean LVEF was 0.37 (range, 0.11 to 0.70), and 19 subjects (41%) had an LVEF of >or= 0.40. Compared to control subjects, EOV subjects had increased left atrial dimension, mitral E-wave velocity, and right heart pressures as well as decreased exercise tidal volume response, functional capacity, rest and exercise end-tidal carbon dioxide, and increased ventilatory equivalent for carbon dioxide and dead space ventilation (all p < 0.05). Multivariate analysis demonstrated atrial fibrillation (odds ratio, 6.7; p = 0.006), digitalis therapy (odds ratio, 0.27; p = 0.02), New York Heart Association class (odds ratio, 3.5; p = 0.0006), rest end-tidal carbon dioxide (odds ratio, 0.87; p = 0.005), and peak heart rate (odds ratio, 0.98; p = 0.02) were independently associated with EOV.
Patients with EOV have clinical characteristics and exercise ventilatory responses consistent with more advanced HF than patients with comparable LV systolic function; EOV may occur in HF patients with an LVEF of >or= 0.40.
心力衰竭(HF)导致的呼吸控制不稳定表现为运动性振荡通气(EOV)。既往对EOV患者的描述未得到对照,且仅限于左心室射血分数(LVEF)≤0.40的受试者。本研究的目的是比较包括EOV受试者与LVEF匹配的HF对照受试者的通气反应在内的临床特征。
从1340例连续接受心肺运动试验的患者中回顾性识别出受试者(n = 47)。研究纳入要求存在EOV,而不考虑LVEF,对照受试者(n = 47)由无EOV且LVEF匹配的HF患者组成。总结并比较每组的特征。
对于EOV受试者,平均LVEF为0.37(范围为0.11至0.70),19名受试者(41%)的LVEF≥0.40。与对照受试者相比,EOV受试者的左心房内径、二尖瓣E波速度和右心压力增加,运动潮气量反应、功能能力、静息和运动末二氧化碳分压降低,二氧化碳通气当量和死腔通气增加(所有p < 0.05)。多变量分析表明,房颤(比值比,6.7;p = 0.006)、洋地黄治疗(比值比,0.27;p = 0.02)、纽约心脏协会分级(比值比,3.5;p = 0.0006)、静息末二氧化碳分压(比值比,0.87;p = 0.005)和峰值心率(比值比,0.98;p = 0.02)与EOV独立相关。
与具有相当左心室收缩功能的患者相比,EOV患者具有与更晚期HF一致的临床特征和运动通气反应;EOV可能发生在LVEF≥0.40的HF患者中。