Rosenthal Ian M, Zhang Ming, Williams Kathy N, Peloquin Charles A, Tyagi Sandeep, Vernon Andrew A, Bishai William R, Chaisson Richard E, Grosset Jacques H, Nuermberger Eric L
Center for Tuberculosis Research, Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, Maryland, United States of America.
PLoS Med. 2007 Dec;4(12):e344. doi: 10.1371/journal.pmed.0040344.
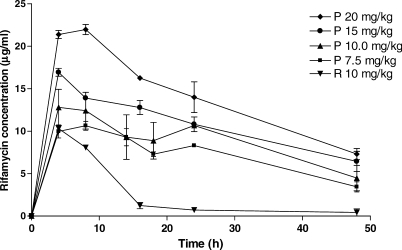
Availability of an ultra-short-course drug regimen capable of curing patients with tuberculosis in 2 to 3 mo would significantly improve global control efforts. Because immediate prospects for novel treatment-shortening drugs remain uncertain, we examined whether better use of existing drugs could shorten the duration of treatment. Rifapentine is a long-lived rifamycin derivative currently recommended only in once-weekly continuation-phase regimens. Moxifloxacin is an 8-methoxyfluoroquinolone currently used in second-line regimens.
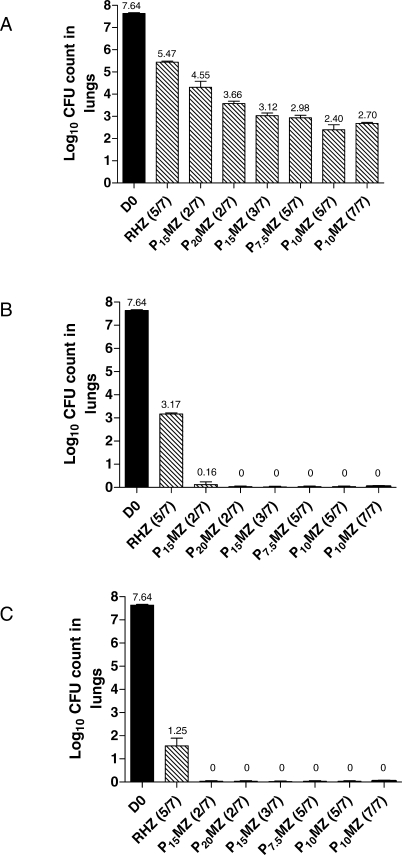
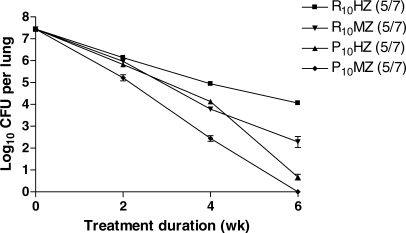
Using a well-established mouse model with a high bacterial burden and human-equivalent drug dosing, we compared the efficacy of rifapentine- and moxifloxacin-containing regimens with that of the standard daily short-course regimen based on rifampin, isoniazid, and pyrazinamide. Bactericidal activity was assessed by lung colony-forming unit counts, and sterilizing activity was assessed by the proportion of mice with culture-positive relapse after 2, 3, 4, and 6 mo of treatment. Here, we demonstrate that replacing rifampin with rifapentine and isoniazid with moxifloxacin dramatically increased the activity of the standard daily regimen. After just 2 mo of treatment, mice receiving rifapentine- and moxifloxacin-containing regimens were found to have negative lung cultures, while those given the standard regimen still harbored 3.17 log10 colony-forming units in the lungs (p < 0.01). No relapse was observed after just 3 mo of treatment with daily and thrice-weekly administered rifapentine- and moxifloxacin-containing regimens, whereas the standard daily regimen required 6 mo to prevent relapse in all mice.
Rifapentine should no longer be viewed solely as a rifamycin for once-weekly administration. Our results suggest that treatment regimens based on daily and thrice-weekly administration of rifapentine and moxifloxacin may permit shortening the current 6 mo duration of treatment to 3 mo or less. Such regimens warrant urgent clinical investigation.
能够在2至3个月内治愈结核病患者的超短程药物方案的出现将显著改善全球防治工作。由于新型缩短治疗时间药物的近期前景仍不确定,我们研究了更好地使用现有药物是否可以缩短治疗时间。利福喷汀是一种长效利福霉素衍生物,目前仅推荐用于每周一次的继续期治疗方案。莫西沙星是一种8-甲氧基氟喹诺酮类药物,目前用于二线治疗方案。
我们使用一个成熟的小鼠模型,该模型具有高细菌载量且药物剂量与人体等效,将含利福喷汀和莫西沙星的治疗方案的疗效与基于利福平、异烟肼和吡嗪酰胺的标准每日短程治疗方案的疗效进行了比较。通过肺菌落形成单位计数评估杀菌活性,并通过治疗2、3、4和6个月后培养阳性复发小鼠的比例评估灭菌活性。在此,我们证明用利福喷汀替代利福平以及用莫西沙星替代异烟肼可显著提高标准每日治疗方案的活性。治疗仅2个月后,接受含利福喷汀和莫西沙星治疗方案的小鼠肺培养物呈阴性,而接受标准治疗方案的小鼠肺中仍有3.17 log10菌落形成单位(p < 0.01)。每日和每周三次给予含利福喷汀和莫西沙星的治疗方案仅治疗3个月后未观察到复发,而标准每日治疗方案需要6个月才能防止所有小鼠复发。
不应再将利福喷汀仅仅视为一种每周一次给药的利福霉素。我们的结果表明,基于每日和每周三次给予利福喷汀和莫西沙星的治疗方案可能允许将目前6个月的治疗时间缩短至3个月或更短。此类方案值得进行紧急临床研究。