Wright Jackson T, Harris-Haywood Sonja, Pressel Sara, Barzilay Joshua, Baimbridge Charles, Bareis Charles J, Basile Jan N, Black Henry R, Dart Richard, Gupta Alok K, Hamilton Bruce P, Einhorn Paula T, Haywood L Julian, Jafri Syed Z A, Louis Gail T, Whelton Paul K, Scott Cranford L, Simmons Debra L, Stanford Carol, Davis Barry R
Department of Medicine, General Clinical Research Center, Cleveland, Ohio, USA.
Arch Intern Med. 2008 Jan 28;168(2):207-17. doi: 10.1001/archinternmed.2007.66.
Antihypertensive drugs with favorable metabolic effects are advocated for first-line therapy in hypertensive patients with metabolic/cardiometabolic syndrome (MetS). We compared outcomes by race in hypertensive individuals with and without MetS treated with a thiazide-type diuretic (chlorthalidone), a calcium channel blocker (amlodipine besylate), an alpha-blocker (doxazosin mesylate), or an angiotensin-converting enzyme inhibitor (lisinopril).
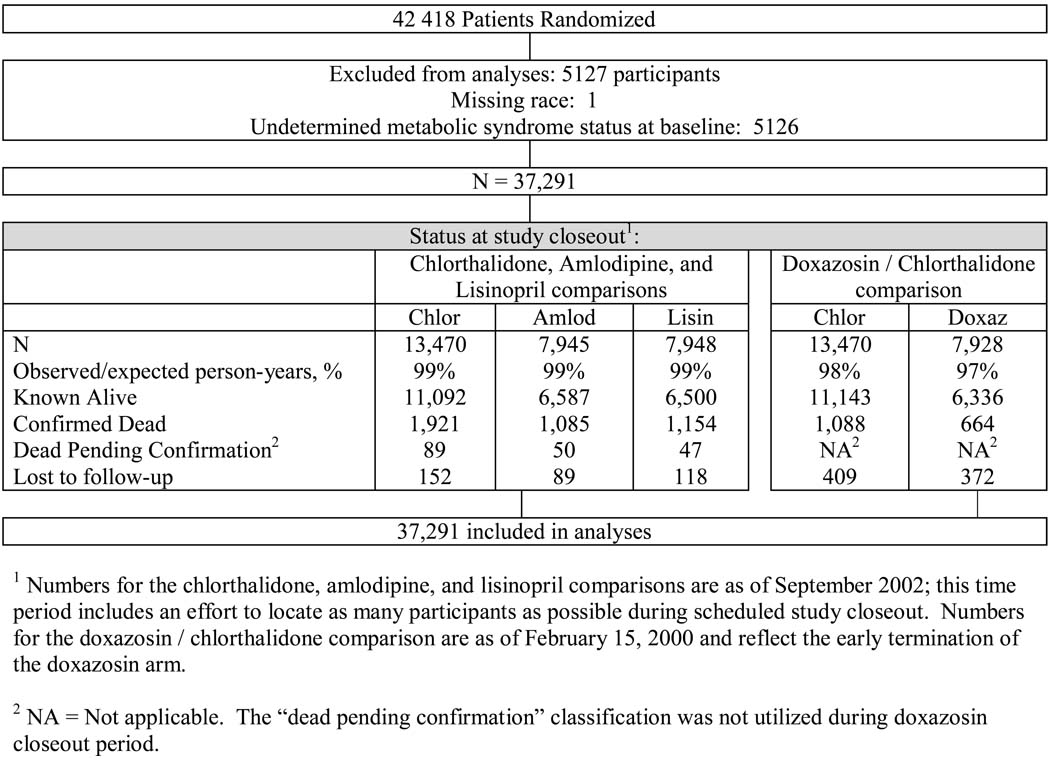
A subgroup analysis of the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT), a randomized, double-blind hypertension treatment trial of 42 418 participants. We defined MetS as hypertension plus at least 2 of the following: fasting serum glucose level of at least 100 mg/dL, body mass index (calculated as weight in kilograms divided by height in meters squared) of at least 30, fasting triglyceride levels of at least 150 mg/dL, and high-density lipoprotein cholesterol levels of less than 40 mg/dL in men or less than 50 mg/dL in women.
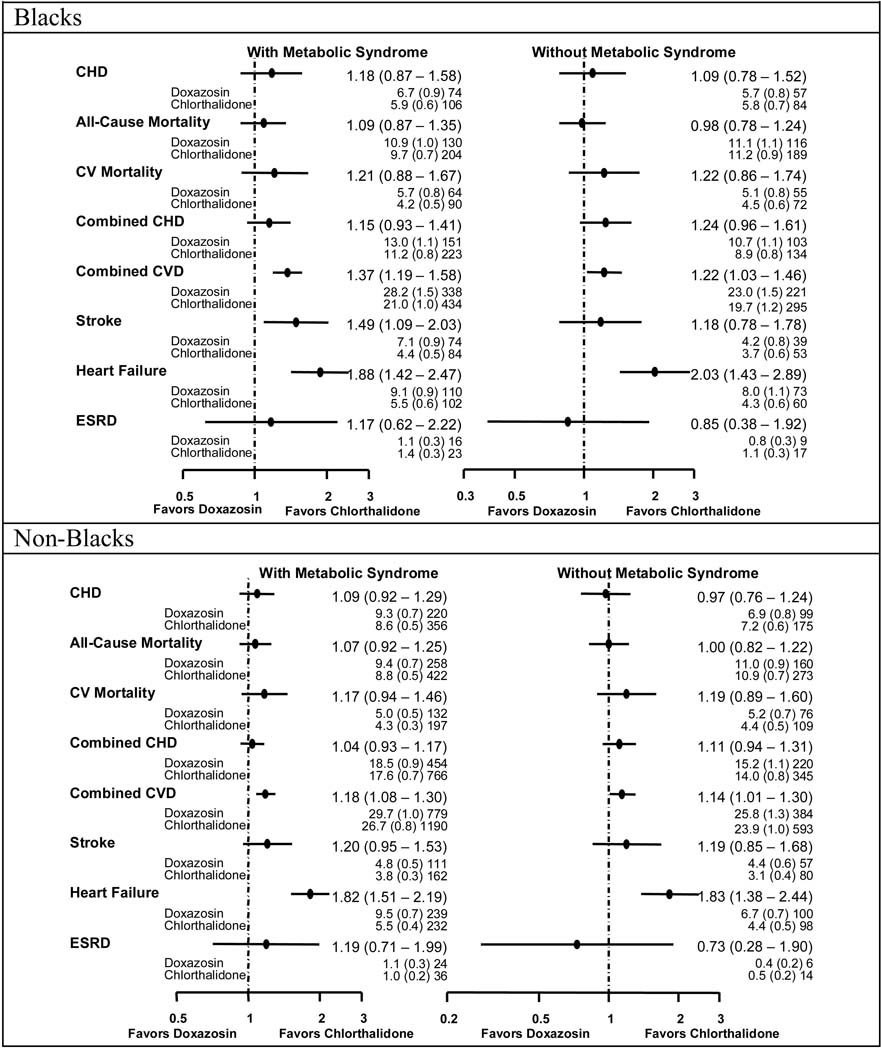
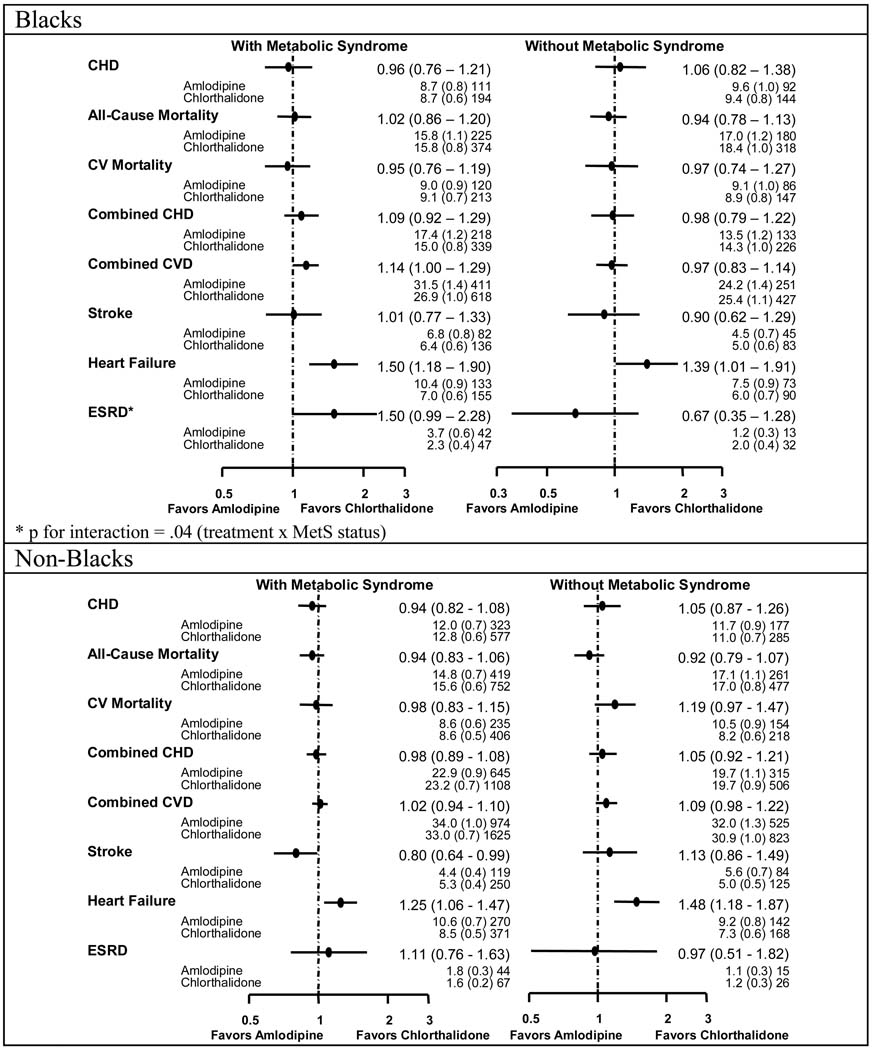
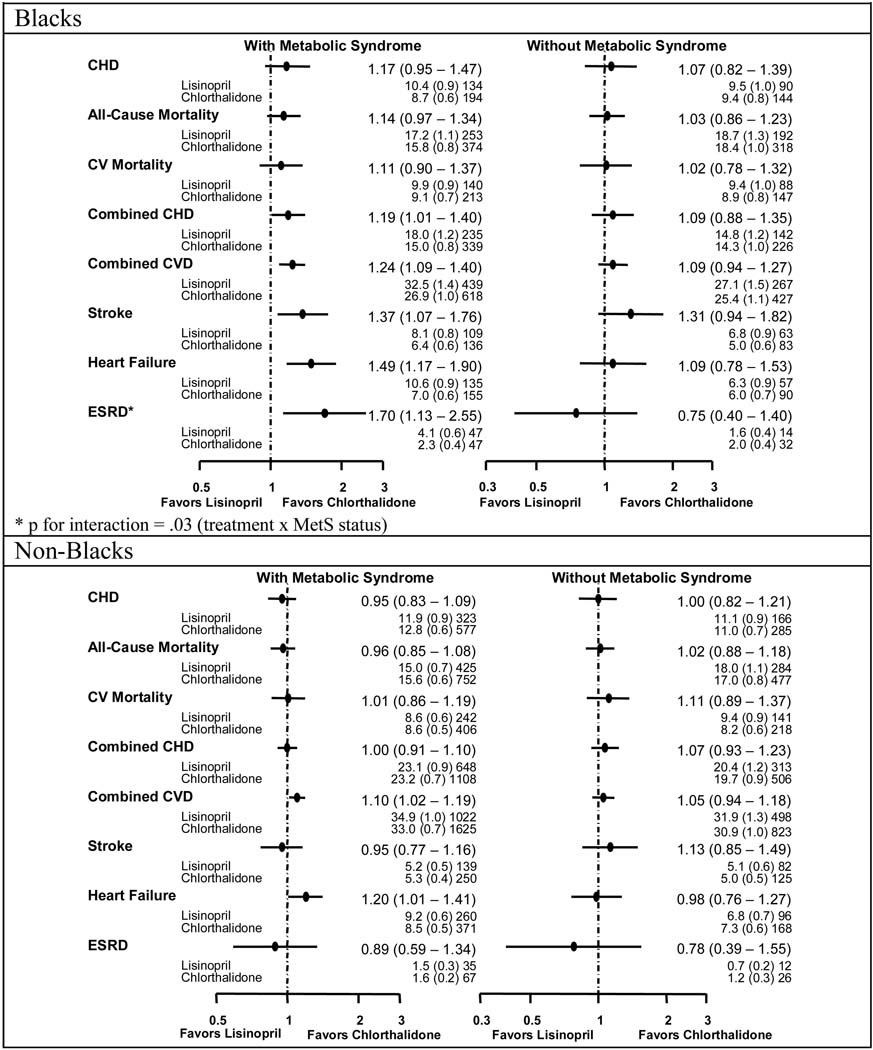
Significantly higher rates of heart failure were consistent across all treatment comparisons in those with MetS. Relative risks (RRs) were 1.50 (95% confidence interval, 1.18-1.90), 1.49 (1.17-1.90), and 1.88 (1.42-2.47) in black participants and 1.25 (1.06-1.47), 1.20 (1.01-1.41), and 1.82 (1.51-2.19) in nonblack participants for amlodipine, lisinopril, and doxazosin comparisons with chlorthalidone, respectively. Higher rates for combined cardiovascular disease were observed with lisinopril-chlorthalidone (RRs, 1.24 [1.09-1.40] and 1.10 [1.02-1.19], respectively) and doxazosin-chlorthalidone comparisons (RRs, 1.37 [1.19-1.58] and 1.18 [1.08-1.30], respectively) in black and nonblack participants with MetS. Higher rates of stroke were seen in black participants only (RR, 1.37 [1.07-1.76] for the lisinopril-chlorthalidone comparison, and RR, 1.49 [1.09-2.03] for the doxazosin-chlorthalidone comparison). Black patients with MetS also had higher rates of end-stage renal disease (RR, 1.70 [1.13-2.55]) with lisinopril compared with chlorthalidone.
The ALLHAT findings fail to support the preference for calcium channel blockers, alpha-blockers, or angiotensin-converting enzyme inhibitors compared with thiazide-type diuretics in patients with the MetS, despite their more favorable metabolic profiles. This was particularly true for black participants.
对于患有代谢/心脏代谢综合征(MetS)的高血压患者,提倡使用具有良好代谢效应的抗高血压药物进行一线治疗。我们比较了使用噻嗪类利尿剂(氯噻酮)、钙通道阻滞剂(苯磺酸氨氯地平)、α受体阻滞剂(甲磺酸多沙唑嗪)或血管紧张素转换酶抑制剂(赖诺普利)治疗的伴有和不伴有MetS的高血压个体按种族划分的治疗结果。
对“抗高血压和降脂治疗预防心脏病发作试验”(ALLHAT)进行亚组分析,这是一项针对42418名参与者的随机、双盲高血压治疗试验。我们将MetS定义为高血压加上以下至少两项:空腹血清葡萄糖水平至少100mg/dL、体重指数(按千克体重除以身高米的平方计算)至少30、空腹甘油三酯水平至少150mg/dL,以及男性高密度脂蛋白胆固醇水平低于40mg/dL或女性低于50mg/dL。
在所有治疗比较中,患有MetS的患者心力衰竭发生率均显著更高。在黑人参与者中,与氯噻酮相比,氨氯地平、赖诺普利和多沙唑嗪的相对风险(RR)分别为1.50(95%置信区间,1.18 - 1.90)、1.49(1.17 - 1.90)和1.88(1.42 - 2.47);在非黑人参与者中,相应的RR分别为1.25(1.06 - 1.47)、1.20(1.01 - 1.41)和1.82(1.51 - 2.19)。在患有MetS的黑人和非黑人参与者中,赖诺普利 - 氯噻酮(RR分别为1.24[1.09 - 1.40]和1.10[1.02 - 1.19])以及多沙唑嗪 - 氯噻酮比较(RR分别为1.37[1.19 - 1.58]和1.18[1.08 - 1.30])时,心血管疾病合并发生率更高。仅在黑人参与者中观察到中风发生率更高(赖诺普利 - 氯噻酮比较的RR为1.37[1.07 - 1.76],多沙唑嗪 - 氯噻酮比较的RR为1.49[1.09 - 2.03])。与氯噻酮相比,患有MetS的黑人患者使用赖诺普利时终末期肾病发生率也更高(RR为1.70[1.13 - 2.55])。
ALLHAT研究结果不支持在患有MetS的患者中,相较于噻嗪类利尿剂,更倾向于使用钙通道阻滞剂、α受体阻滞剂或血管紧张素转换酶抑制剂,尽管它们具有更有利的代谢特征。对于黑人参与者尤其如此。