Rutter Martin K, Wilson Peter W F, Sullivan Lisa M, Fox Caroline S, D'Agostino Ralph B, Meigs James B
Cardiovascular Research Group, Division of Cardiovascular and Endocrine Sciences, University of Manchester, and The Manchester Diabetes Centre, Manchester Royal Infirmary, Manchester, United Kingdom.
Circulation. 2008 Feb 26;117(8):1003-9. doi: 10.1161/CIRCULATIONAHA.107.727727. Epub 2008 Feb 4.
The performance characteristics of surrogate insulin resistance (IR) measures, commonly defined as the top 25% of the measure's distribution, used to predict incident type 2 diabetes mellitus (DM) and cardiovascular disease (CVD) have not been critically assessed in community samples.
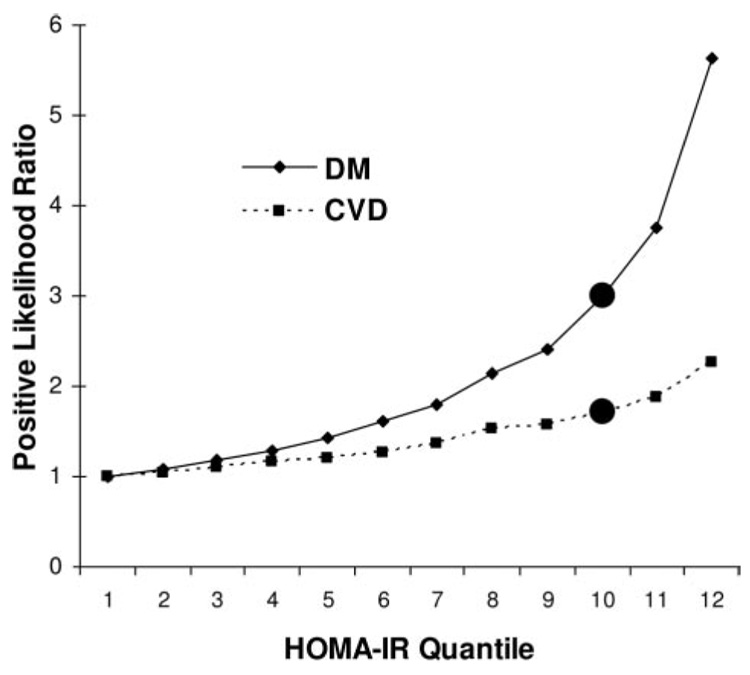
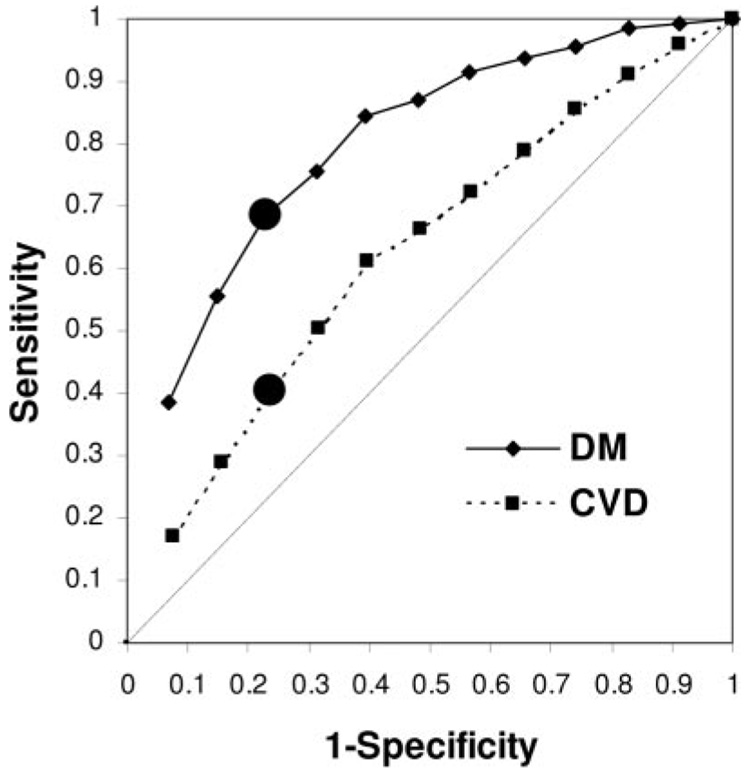
Baseline IR was assessed among 2720 Framingham Offspring Study subjects by use of fasting insulin, the homeostasis model assessment of IR (HOMA-IR), and the reciprocal of the Gutt insulin sensitivity index, with 7- to 11-year follow-up for incident DM (130 cases) or CVD (235). Area under the receiver operating characteristic curve, sensitivity, specificity, and positive likelihood ratio were estimated at 12 diagnostic thresholds (quantiles) of IR measures. Positive likelihood ratios for DM or CVD increased in relation to IR quantiles; risk gradients were greater for DM than for CVD, with no 9th to 10th quantile (76th centile) threshold effects. IR had better discrimination for incident DM than for CVD (HOMA-IR area under the receiver operating characteristic curve: DM 0.80 versus CVD 0.63). The HOMA-IR > or = 76th centile threshold was associated with these test-performance values: sensitivity (DM 68%, CVD 40%), specificity (DM 77%, CVD 76%), and positive likelihood ratio (DM 3.0, CVD 1.7). The HOMA-IR threshold that yielded > 90% sensitivity was the 6th quantile for DM prediction and the 3rd quantile for CVD. Compared with the > or = 76th centile threshold, these alternative thresholds yielded lower specificity (DM 43%, CVD 17%) and positive likelihood ratios (DM 1.6, CVD 1.1).
Surrogate IR measures have modest performance at the 76th centile, with no threshold effects. Different centile thresholds might be selected to optimize sensitivity versus specificity for DM versus CVD prediction if surrogate IR measures are used for risk prediction.
常用于预测2型糖尿病(DM)和心血管疾病(CVD)发病的替代胰岛素抵抗(IR)指标的性能特征,通常定义为该指标分布的前25%,尚未在社区样本中进行严格评估。
在2720名弗雷明汉后代研究受试者中,通过空腹胰岛素、IR的稳态模型评估(HOMA-IR)以及Gutt胰岛素敏感性指数的倒数评估基线IR,并对DM(130例)或CVD(235例)进行7至11年的随访。在IR指标的12个诊断阈值(分位数)处估计受试者工作特征曲线下面积、敏感性、特异性和阳性似然比。DM或CVD的阳性似然比随IR分位数增加;DM的风险梯度大于CVD,且无第9至第10分位数(第76百分位数)阈值效应。IR对DM发病的鉴别能力优于CVD(受试者工作特征曲线下面积:DM为0.80,CVD为0.63)。HOMA-IR≥第76百分位数阈值与以下测试性能值相关:敏感性(DM为68%,CVD为40%)、特异性(DM为77%,CVD为76%)和阳性似然比(DM为3.0,CVD为1.7)。产生>90%敏感性的HOMA-IR阈值在DM预测中为第6分位数,在CVD预测中为第3分位数。与≥第76百分位数阈值相比,这些替代阈值产生的特异性较低(DM为43%,CVD为17%)和阳性似然比(DM为1.6,CVD为1.1)。
替代IR指标在第76百分位数时性能一般,无阈值效应。如果使用替代IR指标进行风险预测,可选择不同的百分位数阈值来优化DM与CVD预测的敏感性与特异性。