Lee C H, Hogan J C, Gibson D G
Cardiac Department, Royal Brompton National Heart and Lung Hospital, London.
Br Heart J. 1991 Apr;65(4):194-200. doi: 10.1136/hrt.65.4.194.
To investigate possible discrepancies between M mode and Doppler echocardiography in assessing early diastolic filling.
Forty seven patients with left ventricular hypertrophy due to aortic stenosis and 26 healthy controls with a similar age range were studied by M mode, Doppler, apexcardiography, and phonocardiography. The patients also underwent cardiac catheterisation. M mode echograms were digitised by a computer. Early diastolic filling in both groups as assessed by the two techniques was compared.
A tertiary cardiac referral centre with facilities for non-invasive and invasive investigations.
Patients referred for assessment of aortic stenosis who had left ventricular hypertrophy.
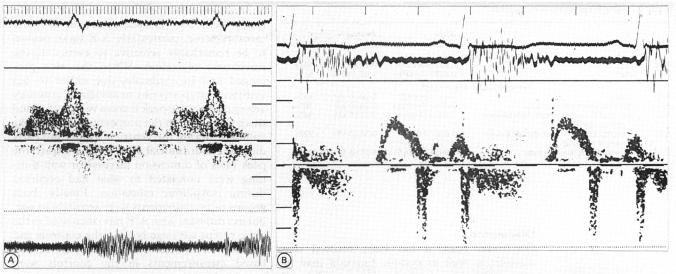
Filling velocities on Doppler and rates of wall thinning and dimension increase on M mode.
Digitised M mode indices of diastolic filling (peak wall thinning rate 6.4 (3.0) v 10.0 (3.0) cm/s and peak rate of dimension increase 9.3 (3.3) v 16 (4.5) cm/s) in the patients and controls were consistently different. In contrast, the Doppler A/E ratio and peak E wave velocity were not; they varied widely among patients with left ventricular hypertrophy. In part, this variability was because the Doppler A/E ratio, but not the digitised M mode indices, was very sensitive to the abnormalities of isovolumic relaxation frequently present in left ventricular hypertrophy. The Doppler A/E ratio varied similarly with age in both normal and hypertrophied hearts; in the patients with ventricular hypertrophy the peak rate of dimension increase depended on age only, whereas the thinning rate was independent of age in both the patients and controls. Neither the A/E ratio nor the M mode indices could be related to the left ventricular end diastolic pressure or the peak aortic pressure difference.
When Doppler and M mode techniques are used to assess rapid filling in patients with left ventricular hypertrophy the M mode indices are more consistently abnormal. The two methods measure different aspects of left ventricular diastolic function and should be regarded as complementary rather than interchangeable.
研究M型和多普勒超声心动图在评估舒张早期充盈方面可能存在的差异。
对47例因主动脉瓣狭窄导致左心室肥厚的患者和26例年龄范围相似的健康对照者进行M型、多普勒、心尖搏动图和心音图检查。患者还接受了心导管检查。M型超声心动图由计算机数字化。比较两组用两种技术评估的舒张早期充盈情况。
一家具备非侵入性和侵入性检查设施的三级心脏转诊中心。
因主动脉瓣狭窄前来评估且有左心室肥厚的患者。
多普勒上的充盈速度以及M型上的室壁变薄率和维度增加率。
患者和对照者的数字化M型舒张期充盈指标(室壁最大变薄率6.4(3.0)对10.0(3.0)cm/s,最大维度增加率9.3(3.3)对16(4.5)cm/s)始终存在差异。相比之下,多普勒A/E比值和E波峰值速度则不然;它们在左心室肥厚患者中差异很大。部分原因在于,多普勒A/E比值,而非数字化M型指标,对左心室肥厚中常见的等容舒张异常非常敏感。正常心脏和肥厚心脏中,多普勒A/E比值随年龄变化相似;在心室肥厚患者中,最大维度增加率仅取决于年龄,而在患者和对照者中,变薄率均与年龄无关。A/E比值和M型指标均与左心室舒张末期压力或主动脉峰值压差无关。
当用多普勒和M型技术评估左心室肥厚患者的快速充盈时,M型指标更一致地表现异常。这两种方法测量左心室舒张功能的不同方面,应视为互补而非可相互替代。