Vasilyev Nikolay V, Melnychenko Ivan, Kitahori Kazuo, Freudenthal Franz P, Phillips Alistair, Kozlik-Feldmann Rainer, Salgo Ivan S, del Nido Pedro J, Bacha Emile A
Department of Cardiac Surgery, Children's Hospital Boston, Harvard Medical School, Boston, Mass 02115, USA.
J Thorac Cardiovasc Surg. 2008 Mar;135(3):603-9. doi: 10.1016/j.jtcvs.2007.09.045.
Safe and effective device closure of ventricular septal defects remains a challenge. We have developed a transcardiac approach to close ventricular septal defects using a patch delivery and fixation system that can be secured under real-time three-dimensional echocardiographic guidance.
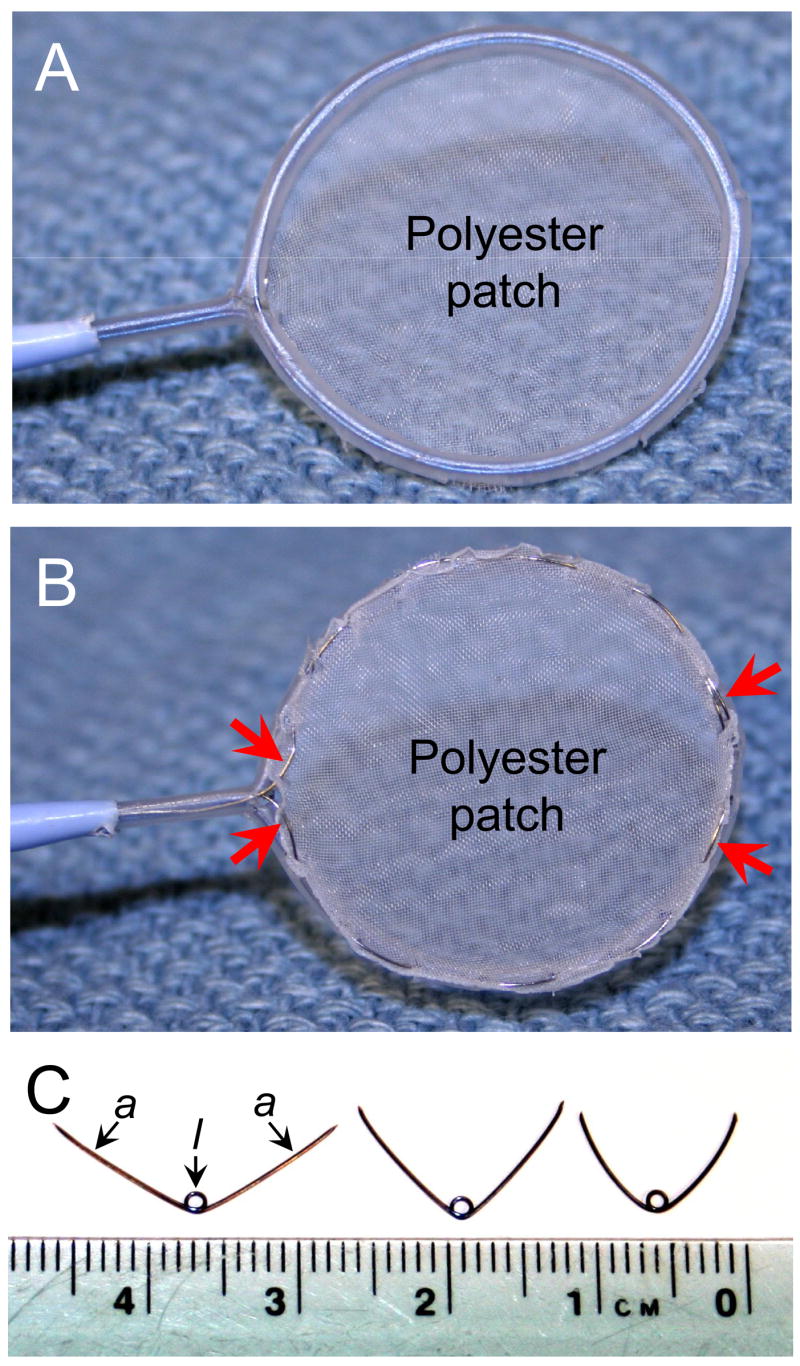
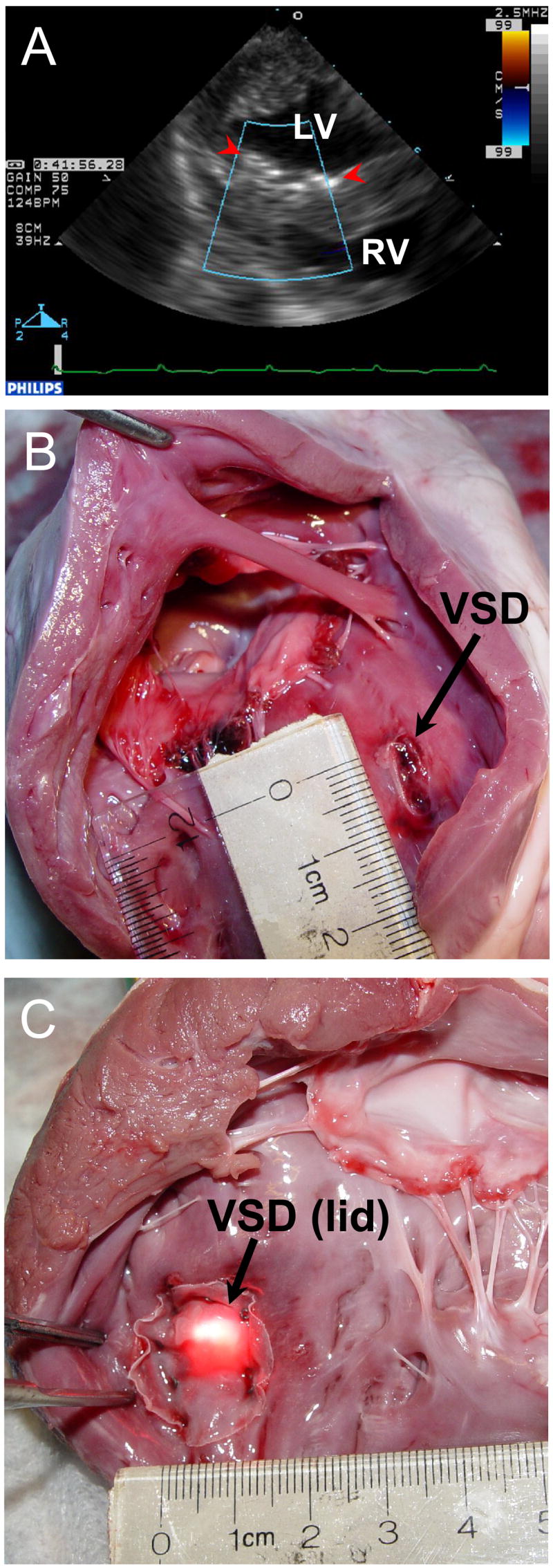
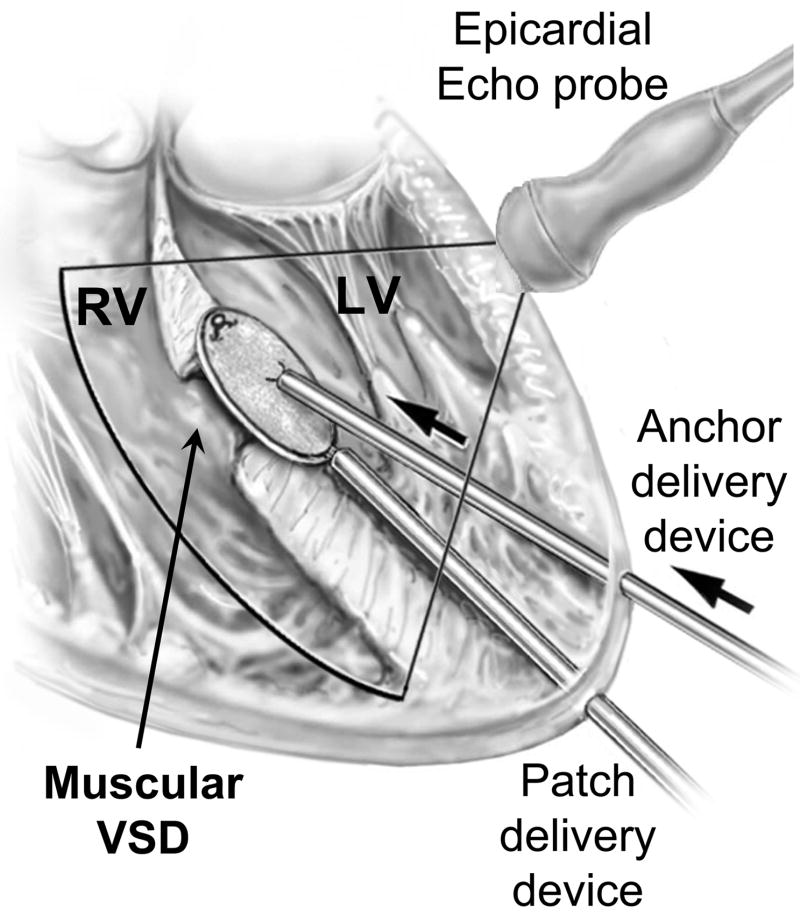
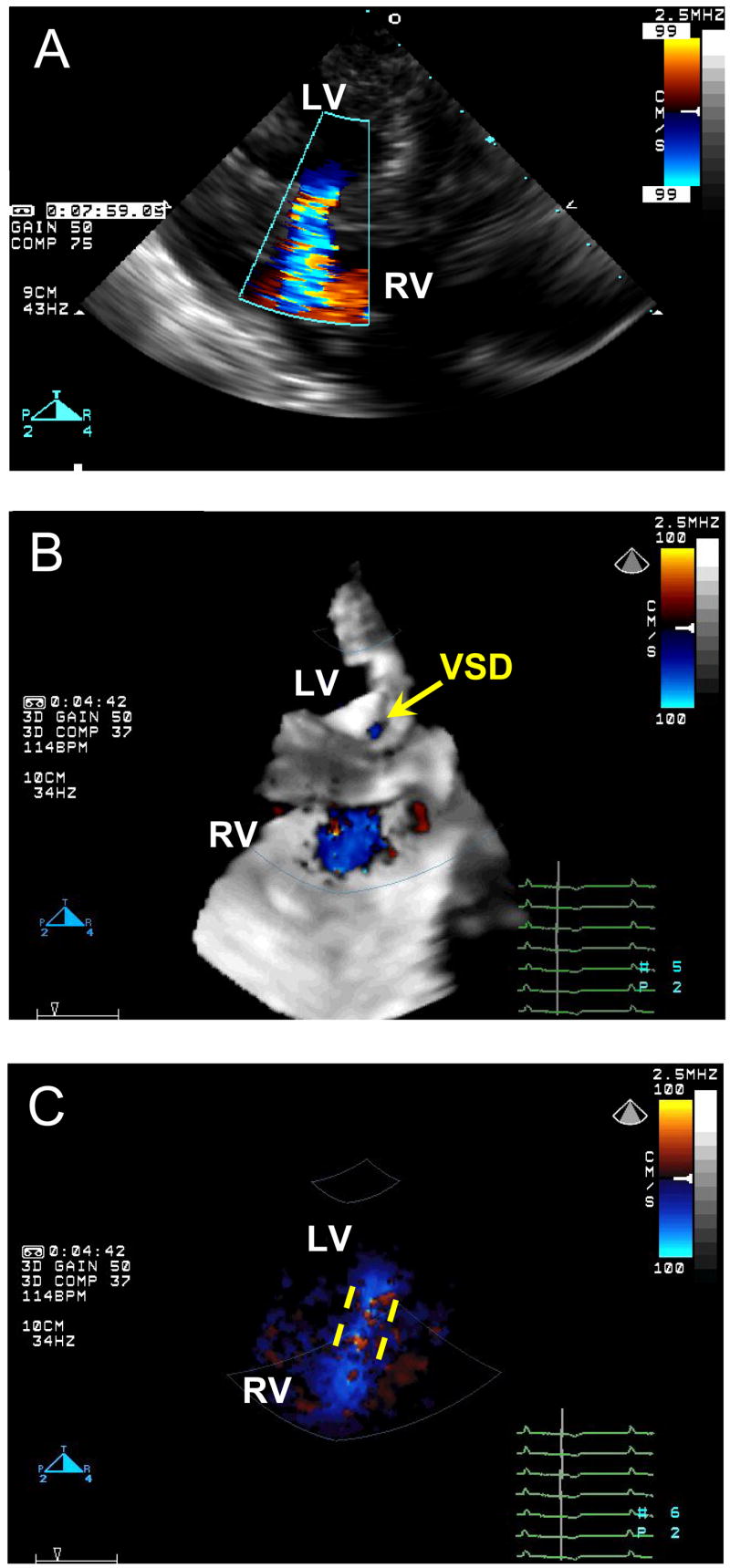
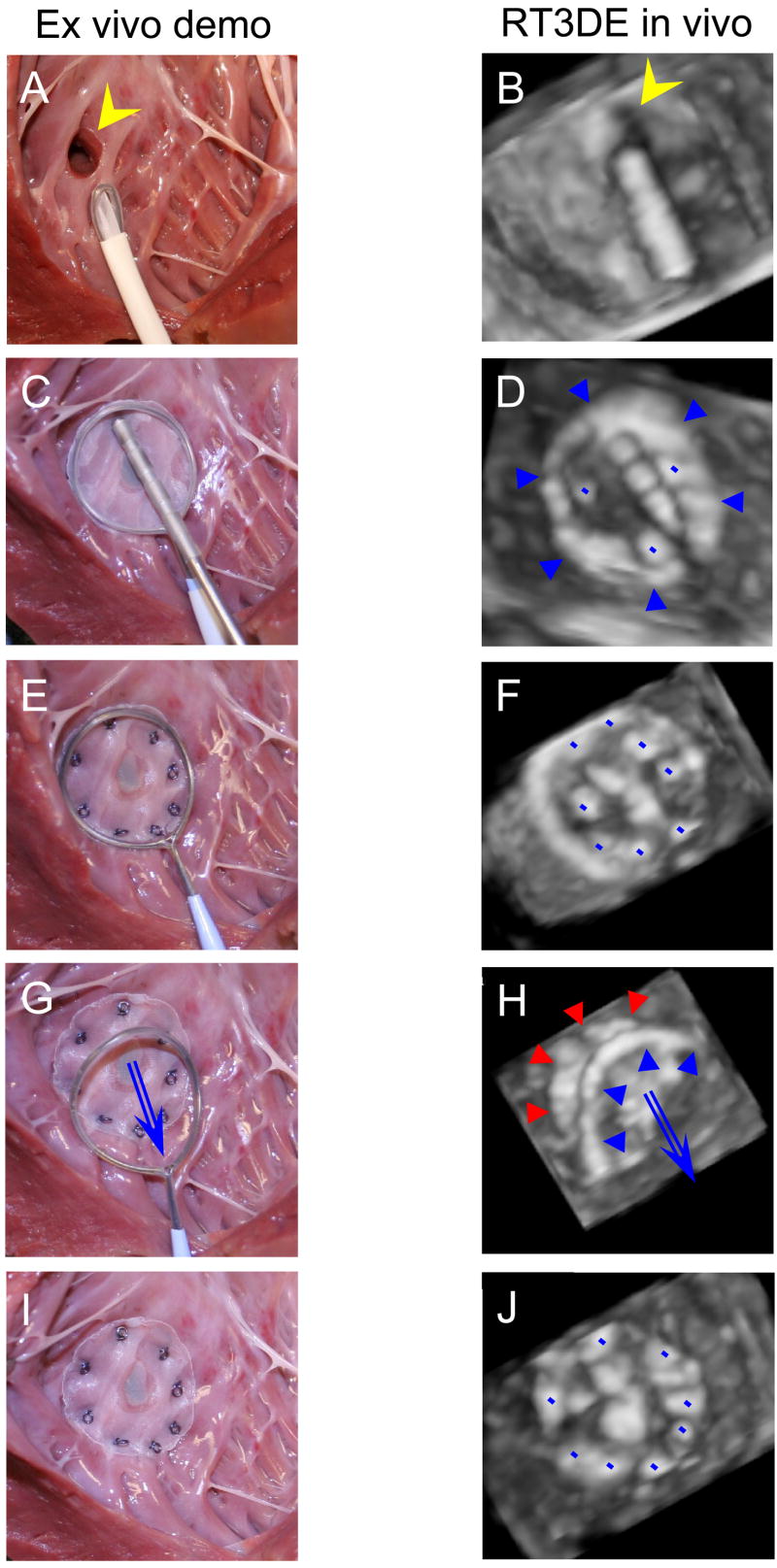
In Yorkshire pigs (n = 8) a coring device was introduced into the left ventricle through a purse-string suture placed on the left ventricular apex, and a muscular ventricular septal defect was created. The patch deployment device containing a 20-mm polyester patch was advanced toward the ventricular septal defect through another purse-string suture on the left ventricular apex, and the patch was deployed under real-time three-dimensional echocardiographic guidance. The anchor delivery device was then introduced into the left ventricle through the first purse-string suture. Nitinol anchors to attach the patch around the ventricular septal defect were deployed under real-time three-dimensional echocardiographic guidance. After patch attachment, residual shunts were sought by means of two-dimensional and three-dimensional color Doppler echocardiography. The heart was then excised, and the septum with the patch was inspected.
A ventricular septal defect was created in the midventricular (n = 4), anterior (n = 2), and apical (n = 2) septum. The mean size was 9.8 mm (8.2-12.0 mm), as determined by means of two-dimensional color Doppler scanning. The ventricular septal defects were completely closed in 7 animals. In one a 2.4-mm residual shunt was identified. No anatomic structures were compromised.
Beating-heart perventricular muscular ventricular septal defect closure without cardiopulmonary bypass can be successfully achieved by using a catheter-based patch delivery and fixation system under real-time three-dimensional echocardiographic guidance. This approach might be a better alternative to cardiac surgery or transcatheter device closure.
安全有效地通过器械闭合室间隔缺损仍是一项挑战。我们研发了一种经心内途径,使用一种可在实时三维超声心动图引导下固定的补片输送与固定系统来闭合室间隔缺损。
在约克郡猪(n = 8)中,通过在左心室心尖处放置的荷包缝线将取芯装置引入左心室,制造一个肌部室间隔缺损。将包含20毫米聚酯补片的补片展开装置通过左心室心尖处的另一根荷包缝线向室间隔缺损推进,并在实时三维超声心动图引导下展开补片。然后将锚定输送装置通过第一根荷包缝线引入左心室。在实时三维超声心动图引导下部署镍钛诺锚,将补片固定在室间隔缺损周围。补片固定后,通过二维和三维彩色多普勒超声心动图寻找残余分流。然后切除心脏,检查带有补片的室间隔。
在室间隔中部(n = 4)、前部(n = 2)和心尖部(n = 2)制造了室间隔缺损。通过二维彩色多普勒扫描测定,平均大小为9.8毫米(8.2 - 12.0毫米)。7只动物的室间隔缺损完全闭合。1只动物发现有2.4毫米的残余分流。没有解剖结构受到损害。
在实时三维超声心动图引导下,使用基于导管的补片输送与固定系统可成功实现不进行体外循环的跳动心脏经心室肌部室间隔缺损闭合。这种方法可能是心脏手术或经导管器械闭合的更好替代方案。