Ther Clin Risk Manag. 2006 Dec;2(4):435-45. doi: 10.2147/tcrm.2006.2.4.435.
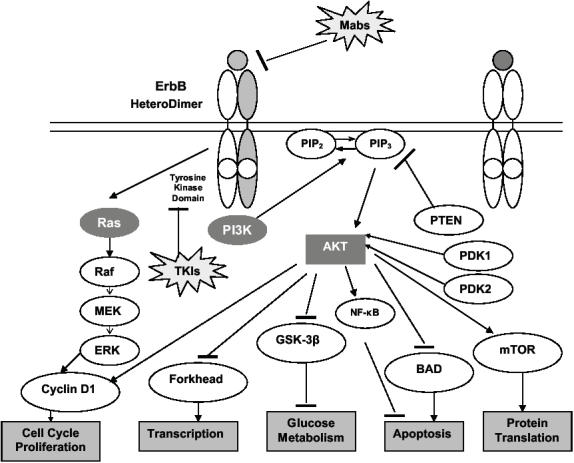
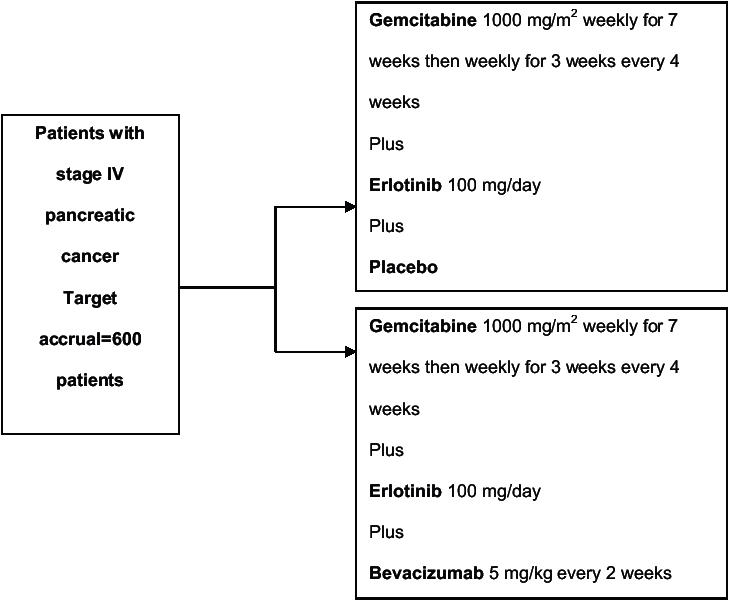
Pancreatic cancer is a largely chemo-resistant disease with a poor prognosis. Despite the adoption of gemcitabine monotherapy as a standard of care, outcomes remain poor. Until recently randomized phase III studies have not demonstrated superiority of various cytotoxic combinations or a number of the newer biologic targeted drugs. The situation has changed with capecitabine and erlotinib, either of which in combination with gemcitabine produces a small increase in survival. Erlotinib is a small molecule tyrosine kinase inhibitor against epidermal growth factor receptor which has an important role in the molecular pathogenesis of pancreatic cancer. In both pre-clinical and early clinical evaluation it has shown anti-tumor activity against pancreatic cancer in combination with gemcitabine. A randomized phase III study in locally advanced and metastatic pancreatic cancer has shown a survival advantage for the combination of gemcitabine plus erlotinib over gemcitabine alone. The rationale for the clinical development of erlotinib in combination with gemcitabine in pancreatic cancer culminating in this randomized trial, together with pharmacologic, toxicity and patient selection considerations form the focus of this review.
胰腺癌是一种主要对化疗耐药的疾病,预后不良。尽管采用吉西他滨单药治疗作为标准治疗方法,但结果仍然不佳。直到最近,随机 III 期研究并未显示出各种细胞毒性联合治疗或一些新型生物靶向药物的优越性。这种情况随着卡培他滨和厄洛替尼的出现而改变,这两种药物中的任何一种与吉西他滨联合使用都能使生存时间略有延长。厄洛替尼是一种针对表皮生长因子受体的小分子酪氨酸激酶抑制剂,在胰腺癌的分子发病机制中具有重要作用。在临床前和早期临床评估中,它已显示出与吉西他滨联合使用时对胰腺癌的抗肿瘤活性。一项针对局部晚期和转移性胰腺癌的随机 III 期研究表明,吉西他滨联合厄洛替尼组的生存优势优于吉西他滨单药组。本文回顾了厄洛替尼联合吉西他滨治疗胰腺癌的临床开发的理论基础,包括药代动力学、毒性和患者选择等方面,这些因素促成了这项随机试验。