Meintjes Graeme, Schoeman Hennie, Morroni Chelsea, Wilson Douglas, Maartens Gary
Division of Infectious Diseases, Department of Medicine, Faculty of Health Sciences, University of Cape Town, Anzio Road, Observatory, 7925, South Africa.
BMC Infect Dis. 2008 May 25;8:72. doi: 10.1186/1471-2334-8-72.
Delay in the diagnosis of tuberculosis (TB) results in excess morbidity and mortality, particularly among HIV-infected individuals. This study was conducted at a secondary level hospital serving communities with a high HIV prevalence in Cape Town, South Africa. The aim was to describe patient and provider delay in the diagnosis of TB in patients with suspected TB requiring admission, and to determine the risk factors for this delay and the consequences.
A cross-sectional study was conducted. Patients admitted who were TB suspects were interviewed using a structured questionnaire to assess history of their symptoms and health seeking behaviour. Data regarding TB diagnosis and outcome were obtained from the medical records. Bivariate associations were described using student's T-tests (for means), chi-square tests (for proportions), and Wilcoxon rank-sum tests (for medians). Linear regression models were used for multivariate analysis.
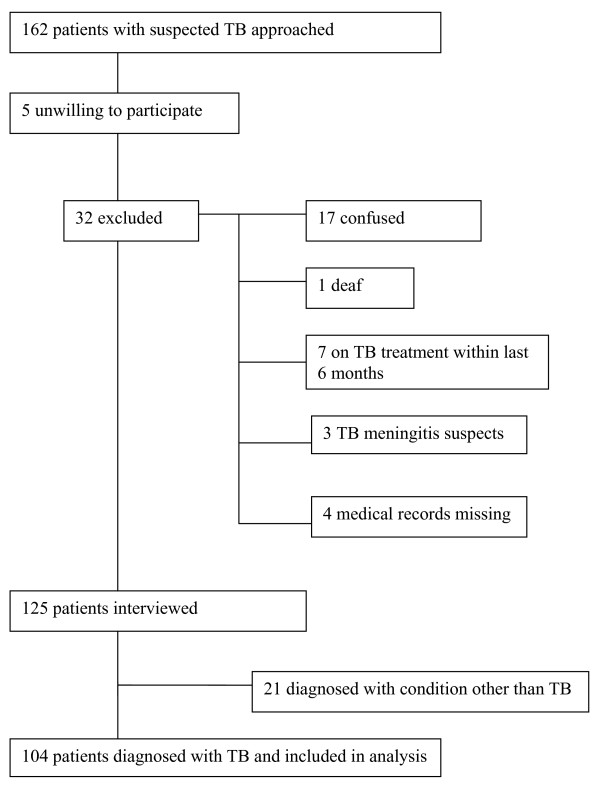
One hundred twenty-five (125) patients were interviewed. In 104 TB was diagnosed and these were included in the analysis. Seventy of 83 (84%) tested were HIV-infected. Provider delay (median = 30 days, interquartile range (IQR) = 10.3-60) was double that of patient delay (median = 14 days, IQR = 7-30). Patients had a median of 3 contacts with formal health care services before referral. Factors independently associated with longer patient delay were male gender, cough and first health care visit being to public sector clinic (compared with private general practitioner). Patient delay > or = 14 days was associated with increased need for transfer to a TB hospital. Provider delay > or = 30 days was associated with increased mortality.
Delay in TB diagnosis was more attributable to provider than patient delay, and provider delay was associated with increased mortality. Interventions to expedite TB diagnosis in primary care need to be developed and evaluated in this setting.
结核病(TB)诊断延误导致发病率和死亡率过高,在艾滋病毒感染者中尤为如此。本研究在南非开普敦一家为艾滋病毒高流行社区服务的二级医院开展。目的是描述疑似结核病且需住院患者的结核病诊断中患者和医护人员的延误情况,确定这种延误的危险因素及其后果。
开展了一项横断面研究。使用结构化问卷对疑似结核病的住院患者进行访谈,以评估其症状史和就医行为。从病历中获取有关结核病诊断和结果的数据。使用学生t检验(用于均值)、卡方检验(用于比例)和威尔科克森秩和检验(用于中位数)描述双变量关联。使用线性回归模型进行多变量分析。
对125名患者进行了访谈。其中104例被诊断为结核病并纳入分析。83例检测者中有70例(84%)感染了艾滋病毒。医护人员延误(中位数 = 30天,四分位间距(IQR) = 10.3 - 60)是患者延误(中位数 = 14天,IQR = 7 - 30)的两倍。患者在转诊前平均与正规医疗服务机构接触3次。与患者较长延误独立相关的因素包括男性、咳嗽以及首次就医是去公共部门诊所(与私人全科医生相比)。患者延误≥14天与转至结核病医院的需求增加有关。医护人员延误≥30天与死亡率增加有关。
结核病诊断延误更多归因于医护人员而非患者延误,且医护人员延误与死亡率增加有关。需要在此环境中制定并评估加快初级保健中结核病诊断的干预措施。