Christo Karla, Prabhakaran Rajani, Lamparello Brooke, Cord Jennalee, Miller Karen K, Goldstein Mark A, Gupta Nupur, Herzog David B, Klibanski Anne, Misra Madhusmita
Massachusetts General Hospital, Neuroendocrine Unit, BUL 457, 55 Fruit St, Boston, MA 02114, USA.
Pediatrics. 2008 Jun;121(6):1127-36. doi: 10.1542/peds.2007-2392.
We hypothesized that, despite increased activity, bone density would be low in athletes with amenorrhea, compared with athletes with eumenorrhea and control subjects, because of associated hypogonadism and would be associated with a decrease in bone formation and increases in bone-resorption markers.
In a cross-sectional study, we examined bone-density measures (spine, hip, and whole body) and body composition by using dual-energy radiograph absorptiometry and assessed fasting levels of insulin-like growth factor I and bone-turnover markers (N-terminal propeptied of type 1 procollagen and N-telopeptide) in 21 athletes with amenorrhea, 18 athletes with eumenorrhea, and 18 control subjects. Subjects were 12 to 18 years of age and of comparable chronologic and bone age.
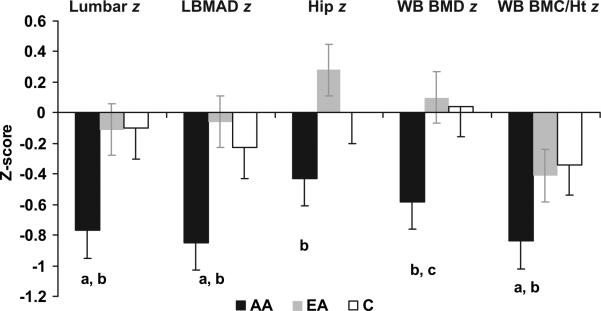
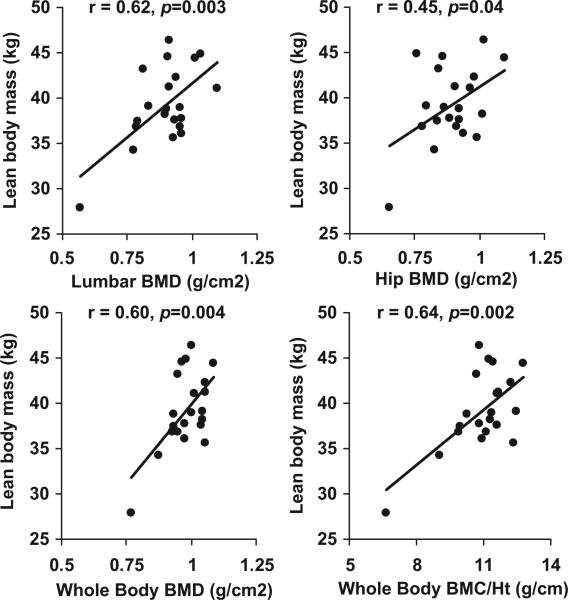
Athletes with amenorrhea had lower bone-density z scores at the spine and whole body, compared with athletes with eumenorrhea and control subjects, and lower hip z scores, compared with athletes with eumenorrhea. Lean mass did not differ between groups. However, athletes with amenorrhea had lower BMI z scores than did athletes with eumenorrhea and lower insulin-like growth factor I levels than did control subjects. Levels of both markers of bone turnover were lower in athletes with amenorrhea than in control subjects. BMI z scores, lean mass, insulin-like growth factor I levels, and diagnostic category were important independent predictors of bone mineral density z scores.
Although they showed no significant differences in lean mass, compared with athletes with eumenorrhea and control subjects, athletes with amenorrhea had lower bone density at the spine and whole body. Insulin-like growth factor I levels, body-composition parameters, and menstrual status were important predictors of bone density. Follow-up studies are necessary to determine whether amenorrhea in athletes adversely affects the rate of bone mass accrual and therefore peak bone mass.
我们推测,尽管闭经运动员的活动量增加,但与月经正常的运动员及对照组相比,由于伴有性腺功能减退,其骨密度会较低,且会与骨形成减少及骨吸收标志物增加有关。
在一项横断面研究中,我们使用双能X线吸收法检查了骨密度测量值(脊柱、髋部和全身)及身体成分,并评估了21名闭经运动员、18名月经正常的运动员和18名对照者空腹时的胰岛素样生长因子I水平及骨转换标志物(I型前胶原N端前肽和N-端肽)。受试者年龄在12至18岁之间,其实际年龄和骨龄相近。
与月经正常的运动员及对照组相比,闭经运动员脊柱和全身的骨密度z值较低,与月经正常的运动员相比,髋部z值也较低。各组间瘦体重无差异。然而,闭经运动员的BMI z值低于月经正常的运动员,胰岛素样生长因子I水平低于对照组。闭经运动员的两种骨转换标志物水平均低于对照组。BMI z值、瘦体重、胰岛素样生长因子I水平及诊断类别是骨矿物质密度z值的重要独立预测因素。
尽管与月经正常的运动员及对照组相比,闭经运动员在瘦体重方面无显著差异,但他们脊柱和全身的骨密度较低。胰岛素样生长因子I水平、身体成分参数及月经状态是骨密度的重要预测因素。有必要进行随访研究,以确定运动员闭经是否会对骨量积累率进而对峰值骨量产生不利影响。