Felley Christian, Perneger Thomas V, Goulet Isabelle, Rouillard Catherine, Azar-Pey Nadereh, Dorta Gian, Hadengue Antoine, Frossard Jean-Louis
Division of Gastroenterology and Hepatology, University Hospitals, and University of Geneva, Geneva, Switzerland.
BMC Gastroenterol. 2008 Jun 3;8:22. doi: 10.1186/1471-230X-8-22.
Little is known about how to most effectively deliver relevant information to patients scheduled for endoscopy.
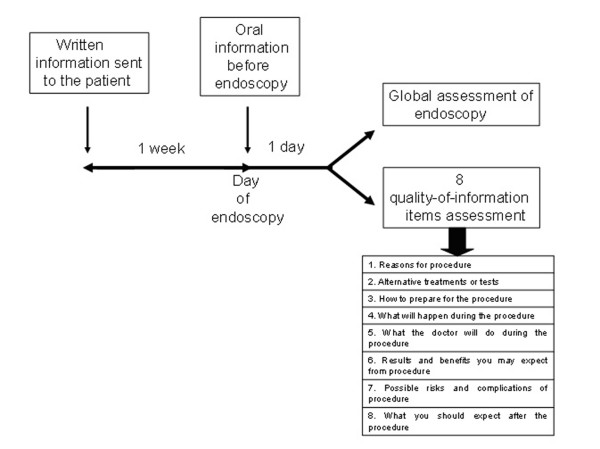
To assess the effects of combined written and oral information, compared with oral information alone on the quality of information before endoscopy and the level of anxiety. We designed a prospective study in two Swiss teaching hospitals which enrolled consecutive patients scheduled for endoscopy over a three-month period. Patients were randomized either to receiving, along with the appointment notice, an explanatory leaflet about the upcoming examination, or to oral information delivered by each patient's doctor. Evaluation of quality of information was rated on scales between 0 (none received) and 5 (excellent). The analysis of outcome variables was performed on the basis of intention to treat-analysis. Multivariate analysis of predictors of information scores was performed by linear regression analysis.
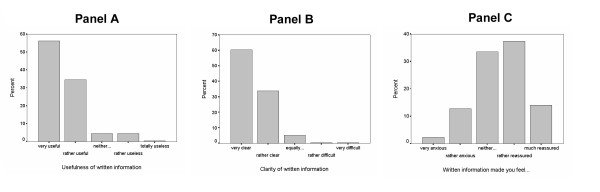
Of 718 eligible patients 577 (80%) returned their questionnaire. Patients who received written leaflets (N = 278) rated the quality of information they received higher than those informed verbally (N = 299), for all 8 quality-of-information items. Differences were significant regarding information about the risks of the procedure (3.24 versus 2.26, p < 0.001), how to prepare for the procedure (3.56 versus 3.23, p = 0.036), what to expect after the procedure (2.99 versus 2.59, p < 0.001), and the 8 quality-of-information items (3.35 versus 3.02, p = 0.002). The two groups reported similar levels of anxiety before procedure (p = 0.66), pain during procedure (p = 0.20), tolerability throughout the procedure (p = 0.76), problems after the procedure (p = 0.22), and overall rating of the procedure between poor and excellent (p = 0.82).
Written information led to more favourable assessments of the quality of information and had no impact on patient anxiety nor on the overall assessment of the endoscopy. Because structured and comprehensive written information is perceived as beneficial by patients, gastroenterologists should clearly explain to their patients the risks, benefits and alternatives of endoscopic procedures.
Current Controlled trial number: ISRCTN34382782.
对于如何最有效地向安排接受内镜检查的患者提供相关信息,我们了解得很少。
为评估书面信息与口头信息相结合,相较于单纯口头信息,对内镜检查前信息质量和焦虑水平的影响。我们在两家瑞士教学医院设计了一项前瞻性研究,在三个月内纳入连续安排接受内镜检查的患者。患者被随机分为两组,一组除预约通知外,还会收到一份关于即将进行检查的解释性传单,另一组由各自的医生提供口头信息。信息质量评估采用0(未收到任何信息)至5(优秀)的量表进行评分。结局变量的分析基于意向性分析。通过线性回归分析对信息得分的预测因素进行多变量分析。
718名符合条件的患者中,577名(80%)返回了问卷。对于所有8项信息质量项目,收到书面传单的患者(N = 278)对所获信息质量的评分高于仅接受口头告知的患者(N = 299)。在关于检查风险的信息方面(3.24对2.26,p < 0.001)、如何为检查做准备方面(3.56对3.23,p = 0.036)、检查后预期方面(2.99对2.59,p < 0.001)以及8项信息质量项目总体方面(3.35对3.02,p = 0.002),差异均具有统计学意义。两组在检查前的焦虑水平(p = 0.66)、检查期间的疼痛程度(p = 0.20)、整个检查过程的耐受性(p = 0.76)、检查后的问题(p = 0.22)以及对检查从差到优的总体评分方面(p = 0.82)报告相似。
书面信息使患者对信息质量的评价更有利,且对患者焦虑及内镜检查的总体评价无影响。由于结构化且全面的书面信息被患者视为有益,胃肠病学家应向患者清楚解释内镜检查的风险、益处及替代方案。
当前对照试验编号:ISRCTN34382782。