Keen John D, Keen James E
Department of Radiology, John H. Stroger Jr. Hospital of Cook County, 1901 West Harrison Street, Chicago, IL 60612-9985, USA.
BMC Med Inform Decis Mak. 2008 Sep 21;8:40. doi: 10.1186/1472-6947-8-40.
In order to promote consumer-oriented informed medical decision-making regarding screening mammography, we created a decision model to predict the age dependence of the cancer detection rate, the recall rate and the secondary performance measures (positive predictive values, total intervention rate, and positive biopsy fraction) for a baseline mammogram.
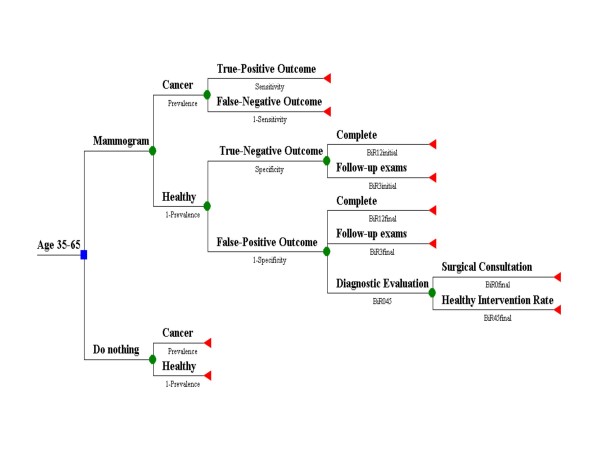
We constructed a decision tree to model the possible outcomes of a baseline screening mammogram in women ages 35 to 65. We compared the single baseline screening mammogram decision with the no screening alternative. We used the Surveillance Epidemiology and End Results national cancer database as the primary input to estimate cancer prevalence. For other probabilities, the model used population-based estimates for screening mammography accuracy and diagnostic mammography outcomes specific to baseline exams. We varied radiologist performance for screening accuracy.
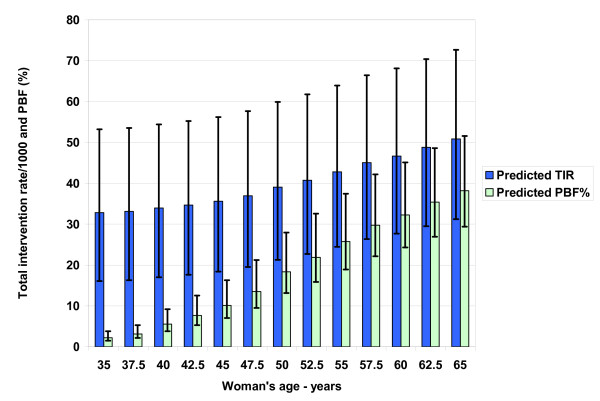
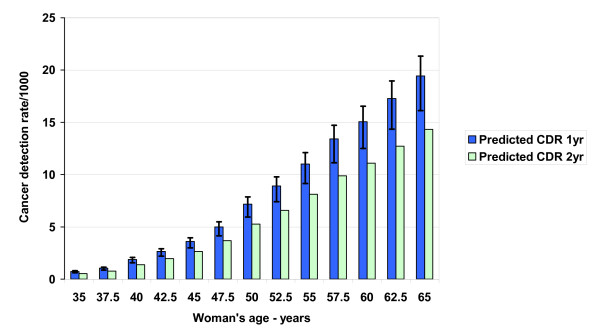
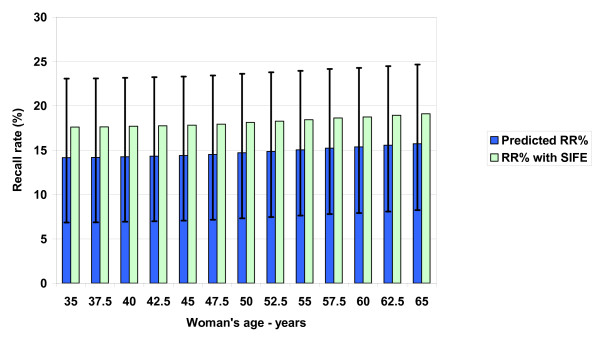
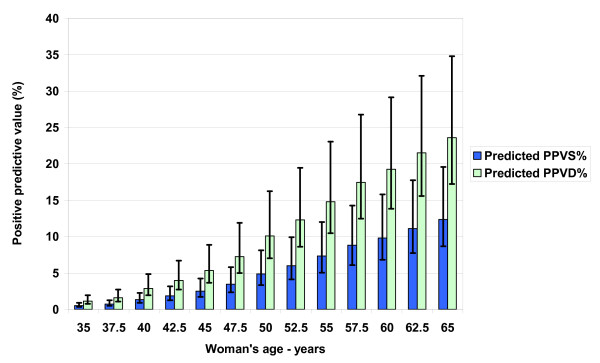
The cancer detection rate increases from 1.9/1000 at age 40 to 7.2/1000 at age 50 to 15.1/1000 at age 60. The recall rate remains relatively stable at 142-157/1000, which varies from 73-236/1000 at age 50 depending on radiologist performance. The positive predictive value of a screening mammogram increases from 1.3% at age 40 to 9.8% at age 60, while the positive predictive value of a diagnostic mammogram varies from 2.9% at age 40 to 19.2% at age 60. The model predicts the total intervention rate = 0.013AGE2 - 0.67AGE + 40, or 34/1000 at age 40 to 47/1000 at age 60. Therefore, the positive biopsy (intervention) fraction varies from 6% at age 40 to 32% at age 60.
Breast cancer prevalence, the cancer detection rate, and all secondary screening mammography performance measures increase substantially with age.
为了促进以消费者为导向的关于乳腺钼靶筛查的明智医疗决策,我们创建了一个决策模型,以预测基线乳腺钼靶检查中癌症检出率、召回率和次要性能指标(阳性预测值、总干预率和阳性活检率)的年龄依赖性。
我们构建了一个决策树,以模拟35至65岁女性基线筛查乳腺钼靶检查的可能结果。我们将单次基线筛查乳腺钼靶检查决策与不进行筛查的选择进行了比较。我们使用监测、流行病学和最终结果国家癌症数据库作为主要输入来估计癌症患病率。对于其他概率,该模型使用基于人群的乳腺钼靶筛查准确性估计值和特定于基线检查的诊断性乳腺钼靶检查结果。我们改变了放射科医生的筛查准确性表现。
癌症检出率从40岁时的1.9/1000增加到50岁时的7.2/1000,再到60岁时的15.1/1000。召回率保持相对稳定,为142 - 157/1000,50岁时根据放射科医生的表现从73 - 236/1000不等。筛查乳腺钼靶检查的阳性预测值从40岁时的1.3%增加到60岁时的9.8%,而诊断性乳腺钼靶检查的阳性预测值从40岁时的2.9%变化到60岁时的19.2%。该模型预测总干预率 = 0.013×年龄² - 0.67×年龄 + 40,即40岁时为34/1000,60岁时为47/1000。因此,阳性活检(干预)率从40岁时的6%变化到60岁时的32%。
乳腺癌患病率、癌症检出率以及所有次要乳腺钼靶筛查性能指标均随年龄大幅增加。