Abeku Tarekegn A, Kristan Mojca, Jones Caroline, Beard James, Mueller Dirk H, Okia Michael, Rapuoda Beth, Greenwood Brian, Cox Jonathan
London School of Hygiene & Tropical Medicine, Keppel Street, London, WC1E 7HT, UK.
Malar J. 2008 Oct 3;7:202. doi: 10.1186/1475-2875-7-202.
The accuracy of malaria diagnosis has received renewed interest in recent years due to changes in treatment policies in favour of relatively high-cost artemisinin-based combination therapies. The use of rapid diagnostic tests (RDTs) based on histidine-rich protein 2 (HRP2) synthesized by Plasmodium falciparum has been widely advocated to save costs and to minimize inappropriate treatment of non-malarial febrile illnesses. HRP2-based RDTs are highly sensitive and stable; however, their specificity is a cause for concern, particularly in areas of intense malaria transmission due to persistence of HRP2 antigens from previous infections.
In this study, 78,454 clinically diagnosed malaria patients were tested using HRP2-based RDTs over a period of approximately four years in four highland sites in Kenya and Uganda representing hypoendemic to mesoendemic settings. In addition, the utility of the tests was evaluated in comparison with expert microscopy for disease management in 2,241 subjects in two sites with different endemicity levels over four months.
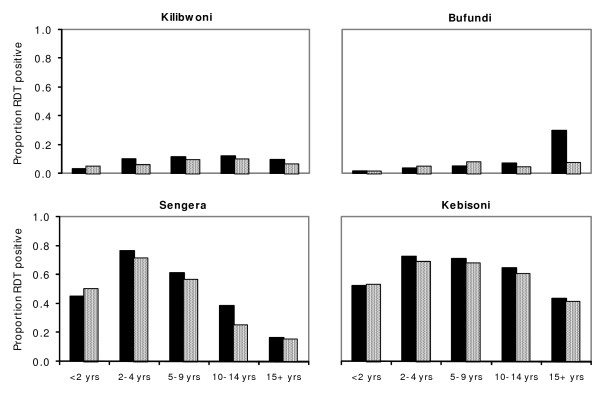
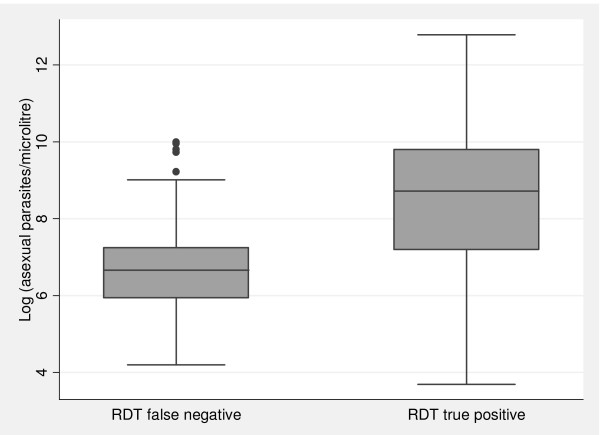
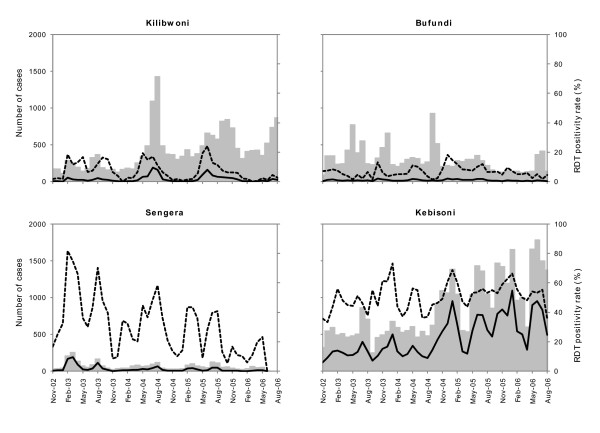
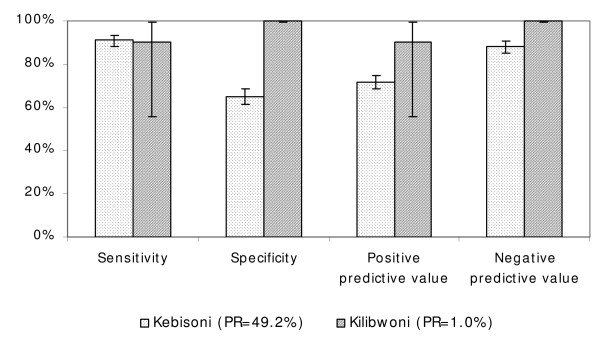
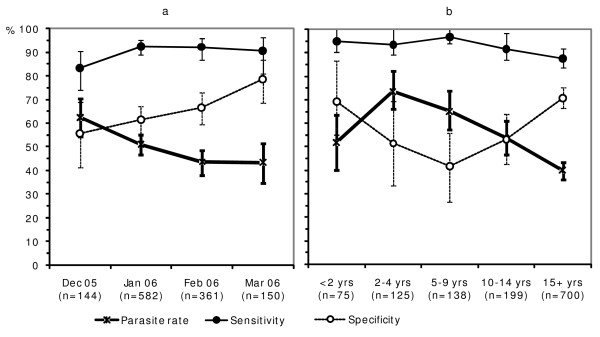
RDT positivity rates varied by season and year, indicating temporal changes in accuracy of clinical diagnosis. Compared to expert microscopy, the sensitivity, specificity, positive predictive value and negative predictive value of the RDTs in a hypoendemic site were 90.0%, 99.9%, 90.0% and 99.9%, respectively. Corresponding measures at a mesoendemic site were 91.0%, 65.0%, 71.6% and 88.1%. Although sensitivities at the two sites were broadly comparable, levels of specificity varied considerably between the sites as well as according to month of test, age of patient, and presence or absence of fever during consultation. Specificity was relatively high in older age groups and increased towards the end of the transmission season, indicating the role played by anti-HRP2 antibodies. Patients with high parasite densities were more likely to test positive with RDTs than those with low density infections.
RDTs may be effective when used in low endemicity situations, but high false positive error rates may occur in areas with moderately high transmission. Reports on specificity of RDTs and cost-effectiveness analyses on their use should be interpreted with caution as there may be wide variations in these measurements depending upon endemicity, season and the age group of patients studied.
近年来,由于治疗政策转向采用成本相对较高的青蒿素联合疗法,疟疾诊断的准确性重新受到关注。基于恶性疟原虫合成的富含组氨酸蛋白2(HRP2)的快速诊断测试(RDT)被广泛提倡用于节省成本并尽量减少对非疟疾发热疾病的不恰当治疗。基于HRP2的RDT高度敏感且稳定;然而,其特异性令人担忧,特别是在疟疾传播强烈的地区,因为既往感染产生的HRP2抗原会持续存在。
在本研究中,在肯尼亚和乌干达的四个高地地区(代表低流行至中流行环境),对约78454例临床诊断为疟疾的患者在大约四年的时间里使用基于HRP2的RDT进行检测。此外,在四个月内,在两个不同流行程度的地区,对2241名受试者进行检测,将这些测试与专家显微镜检查进行比较,以评估其在疾病管理中的效用。
RDT阳性率随季节和年份变化,表明临床诊断准确性的时间变化。与专家显微镜检查相比,在低流行地区,RDT的敏感性、特异性、阳性预测值和阴性预测值分别为90.0%、99.9%、90.0%和99.9%。在中流行地区相应的指标分别为91.0%、65.0%、71.6%和88.1%。虽然两个地区的敏感性大致相当,但不同地区以及根据检测月份、患者年龄和就诊时是否发热,特异性水平差异很大。老年组的特异性相对较高,且在传播季节末期升高,表明抗HRP2抗体发挥的作用。寄生虫密度高的患者比低密度感染患者更有可能RDT检测呈阳性。
RDT在低流行情况下使用可能有效,但在传播程度中等偏高的地区可能会出现较高的假阳性错误率。关于RDT特异性的报告及其使用的成本效益分析应谨慎解读,因为这些测量可能因流行程度、季节和所研究患者的年龄组而有很大差异。