Mshani Issa H, Jackson Frank M, Minja Elihaika G, Abbasi Said, Lilolime Nasoro S, Makala Faraja E, Lazaro Alfred B, Mchola Idrisa S, Mukabana Linda N, Kahamba Najat F, Limwagu Alex J, Njalambaha Rukia M, Ngowo Halfan S, Bisanzio Donal, Baldini Francesco, Babayan Simon A, Okumu Fredros
Environmental Health, and Ecological Sciences Department, Ifakara Health Institute, Morogoro, United Republic of Tanzania.
School of Biodiversity, One Health and Veterinary Medicine, The University of Glasgow, Glasgow, UK.
Malar J. 2024 Dec 18;23(1):376. doi: 10.1186/s12936-024-05191-8.
Malaria-endemic countries are increasingly adopting data-driven risk stratification, often at district or higher regional levels, to guide their intervention strategies. The data typically comes from population-level surveys collected by rapid diagnostic tests (RDTs), which unfortunately perform poorly in low transmission settings. Here, a high-resolution survey of Plasmodium falciparum prevalence rate (PfPR) was conducted in two Tanzanian districts using rapid diagnostic tests (RDTs), microscopy, and quantitative polymerase chain reaction (qPCR) assays, enabling the comparison of fine-scale strata derived from these different diagnostic methods.
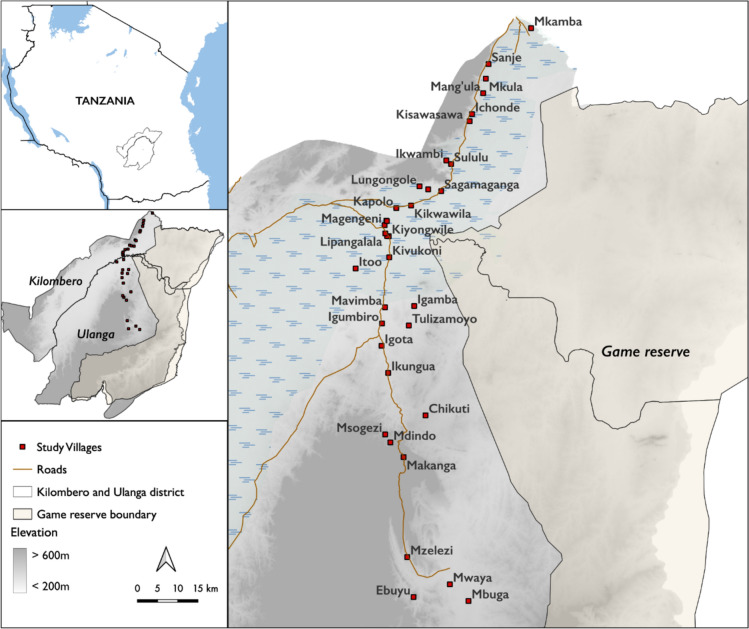
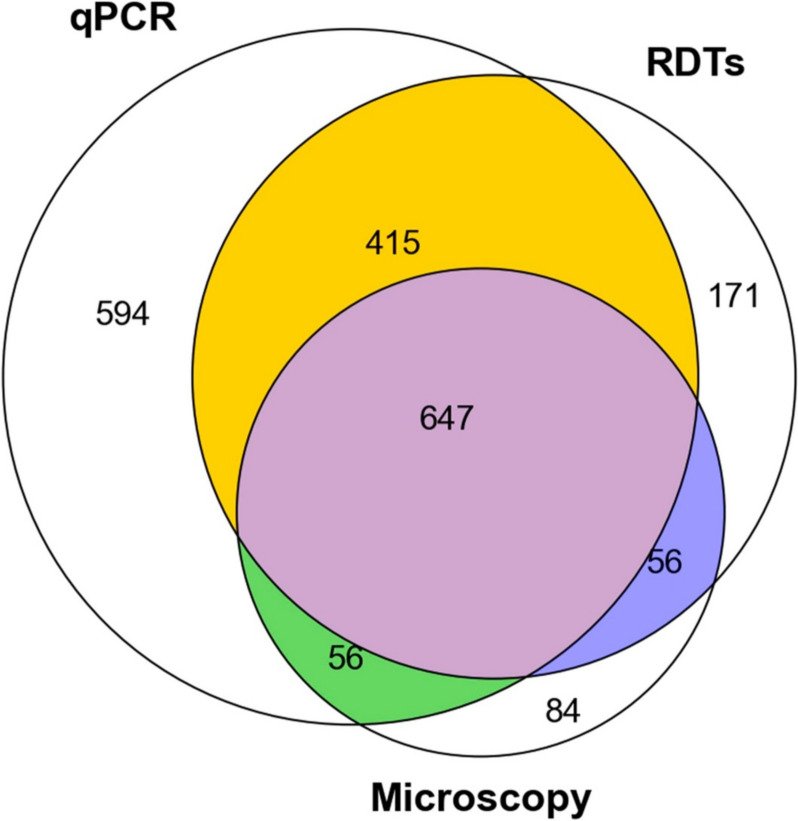
A cross-sectional survey was conducted in 35 villages in Ulanga and Kilombero districts, south-eastern Tanzania between 2022 and 2023. A total of 7,628 individuals were screened using RDTs (SD-BIOLINE) and microscopy, with two thirds of the samples further analysed by qPCR. The data was used to categorize each district and village as having very low (PfPR < 1%), low (1%≤PfPR < 5%), moderate (5%≤PfPR < 30%), or high (PfPR ≥ 30%) parasite prevalence. A generalized linear mixed model was used to analyse infection risk factors. Other metrics, including positive predictive value (PPV), sensitivity, specificity, parasite densities, and Kappa statistics were computed for RDTs or microscopy and compared to qPCR as reference.
Significant fine-scale variations in malaria risk were observed within and between the districts, with village prevalence ranging from 0% to > 50%. Prevalence varied by testing method: Kilombero was low risk by RDTs (PfPR = 3%) and microscopy (PfPR = 2%) but moderate by qPCR (PfPR = 9%); Ulanga was high risk by RDTs (PfPR = 39%) and qPCR (PfPR = 54%) but moderate by microscopy (PfPR = 26%). RDTs and microscopy classified majority of the 35 villages as very low to low risk (18-21 villages). In contrast, qPCR classified most villages as moderate to high risk (29 villages). Using qPCR as the reference, PPV for RDTs and microscopy ranged from as low as < 20% in very low transmission villages to > 80% in moderate and high transmission villages. Sensitivity was 62% for RDTs and 41% for microscopy; specificity was 93% and 96%, respectively. Kappa values were 0.7 for RDTs and 0.5 for microscopy. School-age children (5-15 years) had higher malaria prevalence and parasite densities than adults (P < 0.001). High-prevalence villages also had higher parasite densities (Spearman r = 0.77, P < 0.001 for qPCR; r = 0.55, P = 0.003 for microscopy).
This study highlights significant fine-scale variability in malaria burden within and between the study districts and emphasizes the variable performance of the testing methods when stratifying risk at local scales. While RDTs and microscopy were effective in high-transmission areas, they performed poorly in low-transmission settings; and classified most villages as very low or low risk. In contrast, qPCR classified most villages as moderate or high risk. The findings emphasize that, where precise mapping and effective targeting of malaria are required in localized settings, tests must be both operationally feasible and highly sensitive. Furthermore, when planning microstratification efforts to guide local control measures, it is crucial to carefully consider both the strengths and limitations of the available data and the testing methods employed.
疟疾流行国家越来越多地采用数据驱动的风险分层方法,通常在地区或更高区域层面,以指导其干预策略。数据通常来自快速诊断检测(RDT)收集的人群层面调查,不幸的是,在低传播环境中其表现不佳。在此,使用快速诊断检测(RDT)、显微镜检查和定量聚合酶链反应(qPCR)检测法,在坦桑尼亚的两个地区进行了一项关于恶性疟原虫流行率(PfPR)的高分辨率调查,从而能够比较源自这些不同诊断方法的精细分层。
2022年至2023年期间,在坦桑尼亚东南部的乌兰加和基洛梅罗地区的35个村庄进行了横断面调查。使用RDT(SD - BIOLINE)和显微镜检查对总共7628人进行了筛查,三分之二的样本进一步通过qPCR进行分析。数据用于将每个地区和村庄分类为寄生虫流行率极低(PfPR < 1%)、低(1%≤PfPR < 5%)、中等(5%≤PfPR < 30%)或高(PfPR≥30%)。使用广义线性混合模型分析感染风险因素。针对RDT或显微镜检查计算了其他指标,包括阳性预测值(PPV)、敏感性、特异性、寄生虫密度和kappa统计量,并与作为参考的qPCR进行比较。
在各地区内部和之间观察到疟疾风险存在显著的精细尺度变化,村庄流行率范围从0%到>50%。流行率因检测方法而异:基洛梅罗地区通过RDT(PfPR = 3%)和显微镜检查(PfPR = 2%)显示为低风险,但通过qPCR为中等风险(PfPR = 9%);乌兰加地区通过RDT(PfPR = 39%)和qPCR(PfPR = 54%)显示为高风险,但通过显微镜检查为中等风险(PfPR = 26%)。RDT和显微镜检查将35个村庄中的大多数分类为极低到低风险(18 - 21个村庄)。相比之下,qPCR将大多数村庄分类为中等至高风险(29个村庄)。以qPCR作为参考,RDT和显微镜检查的PPV范围从极低传播村庄的低至<20%到中等和高传播村庄的>80%。RDT的敏感性为62%,显微镜检查为41%;特异性分别为93%和96%。RDT的kappa值为0.7,显微镜检查为0.5。学龄儿童(5 - 15岁)的疟疾流行率和寄生虫密度高于成年人(P < 0.001)。高流行村庄的寄生虫密度也更高(qPCR的Spearman r = 0.77,P < 0.001;显微镜检查的r = 0.55,P = 0.003)。
本研究突出了研究地区内部和之间疟疾负担存在显著的精细尺度变异性,并强调了在局部尺度分层风险时检测方法的可变性能。虽然RDT和显微镜检查在高传播地区有效,但在低传播环境中表现不佳;并且将大多数村庄分类为极低或低风险。相比之下,qPCR将大多数村庄分类为中等或高风险。研究结果强调,在需要对疟疾进行精确绘图和有效靶向的局部环境中,检测方法必须在操作上可行且高度敏感。此外,在规划微观分层努力以指导地方控制措施时,仔细考虑现有数据和所采用检测方法的优势和局限性至关重要。