Kirchhoff Chlodwig, Braunstein Volker, Kirchhoff Sonja, Sprecher Christoph M, Ockert Ben, Fischer Florian, Leidel Bernd A, Biberthaler Peter
Department of Orthopedic Sports Surgery, Technische Universitaet Muenchen, Connollystrasse 32, D-80809 Munich, Germany.
BMC Musculoskelet Disord. 2008 Oct 12;9:138. doi: 10.1186/1471-2474-9-138.
Concerning surgical management experience with locking plates for proximal humeral fractures has been described with promising results. Though, distinct hardware related complaints after fracture union are reported. Information concerning the outcome after removal of hardware from the proximal humerus is lacking and most studies on hardware removal are focused on the lower extremity. Therefore the aim of this study was to analyze the functional short-term outcome following removal of locking plate fixation of the proximal humerus.
Patients undergoing removal of a locking plate of the proximal humerus were prospectively followed. Patients were subdivided into the following groups: Group HI: symptoms of hardware related subacromial impingement, Group RD: persisting rotation deficit, Group RQ: patients with request for a hardware removal. The clinical (Constant-Murley score) and radiologic (AP and axial view) follow-up took place three and six months after the operation. To evaluate subjective results, the Medical Outcomes Study Short Form-36 (SF-36), was completed.
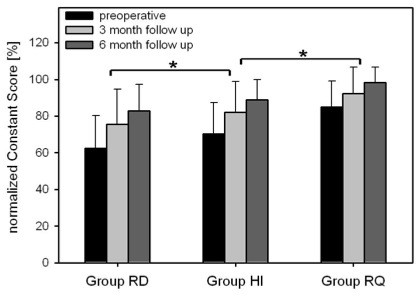
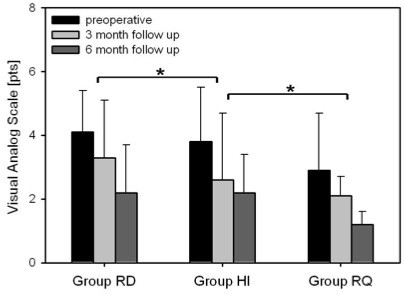
59 patients were included. The mean length of time with the hardware in place was 15.2 +/- 3.81 months. The mean of the adjusted overall Constant score before hardware removal was 66.2 +/- 25.2% and increased significantly to 73.1 +/- 22.5% after 3 months; and to 84.3 +/- 20.6% after 6 months (p < 0.001). The mean of preoperative pain on the VAS-scale before hardware removal was 5.2 +/- 2.9, after 6 months pain in all groups decreased significantly (p < 0.001). The SF-36 physical component score revealed a significant overall improvement in both genders (p < 0.001) at six months.
A significant improvement of clinical outcome following removal was found. However, a general recommendation for hardware removal is not justified, as the risk of an anew surgical and anesthetic procedure with all possible complications has to be carefully taken into account. However, for patients with distinct symptoms it might be justified.
关于使用锁定钢板治疗肱骨近端骨折的手术管理经验已有报道,结果令人满意。然而,有报道称骨折愈合后出现了与硬件相关的明显不适。目前缺乏关于从肱骨近端取出硬件后的结果的信息,并且大多数关于硬件取出的研究都集中在下肢。因此,本研究的目的是分析肱骨近端锁定钢板固定取出后的短期功能结果。
对接受肱骨近端锁定钢板取出术的患者进行前瞻性随访。患者被分为以下几组:HI组:与硬件相关的肩峰下撞击症状;RD组:持续的旋转功能障碍;RQ组:要求取出硬件的患者。术后3个月和6个月进行临床(Constant-Murley评分)和放射学(前后位和轴位视图)随访。为了评估主观结果,完成了医学结局研究简表36(SF-36)。
纳入59例患者。硬件在位的平均时间为15.2±3.81个月。取出硬件前调整后的总体Constant评分平均为66.2±25.2%,3个月后显著提高至73.1±22.5%;6个月后提高至84.3±20.6%(p<0.001)。取出硬件前VAS量表上的术前平均疼痛评分为5.2±2.9,6个月后所有组的疼痛均显著降低(p<0.001)。SF-36身体成分评分显示,6个月时男女总体均有显著改善(p<0.001)。
发现取出硬件后临床结果有显著改善。然而,由于必须仔细考虑再次手术和麻醉程序以及所有可能并发症的风险,因此不建议普遍取出硬件。然而,对于有明显症状的患者,取出硬件可能是合理的。