Pekkan Kerem, Dasi Lakshimi P, de Zélicourt Diane, Sundareswaran Kartik S, Fogel Mark A, Kanter Kirk R, Yoganathan Ajit P
Department of Biomedical Engineering, Carnegie Mellon University, Pittsburgh, PA, USA.
Ann Biomed Eng. 2009 Jan;37(1):50-63. doi: 10.1007/s10439-008-9591-z. Epub 2008 Nov 6.
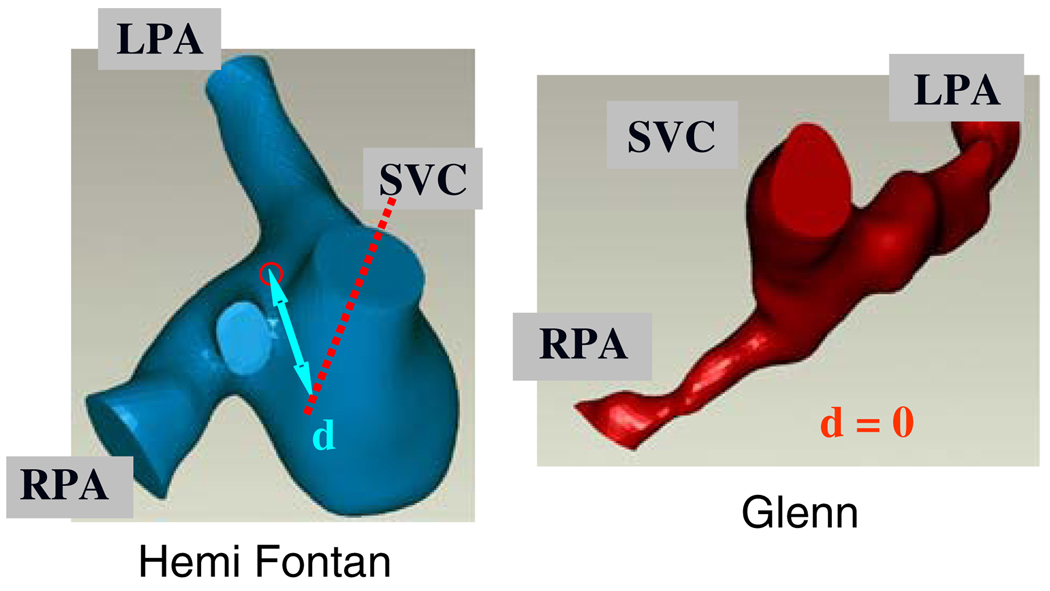
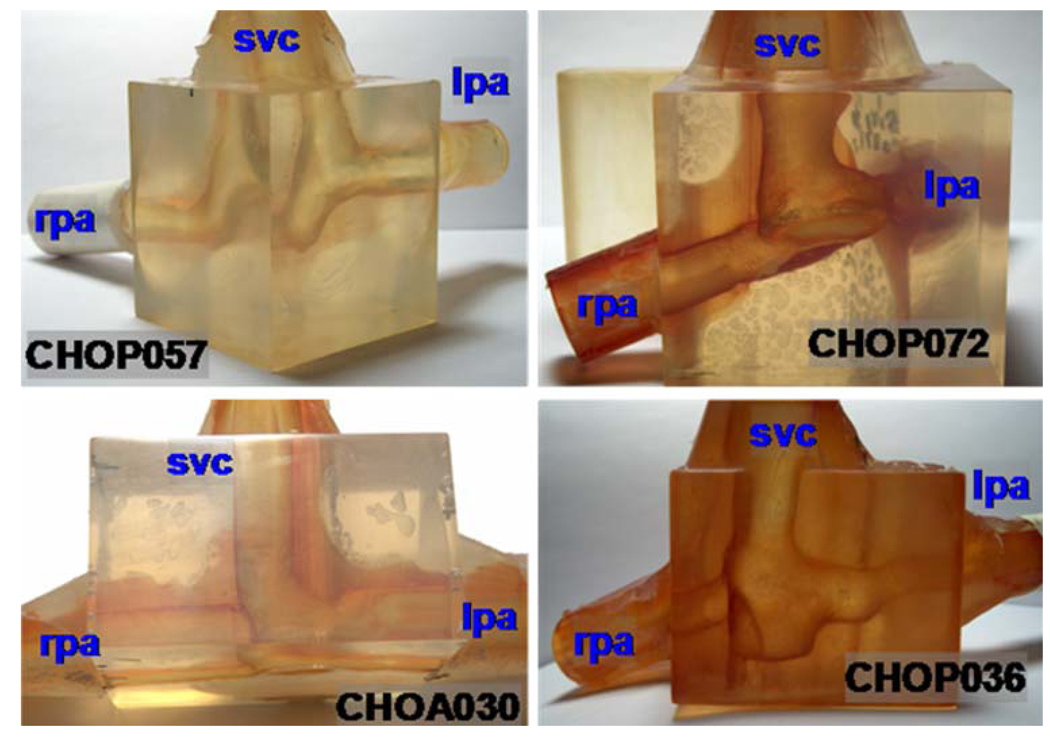
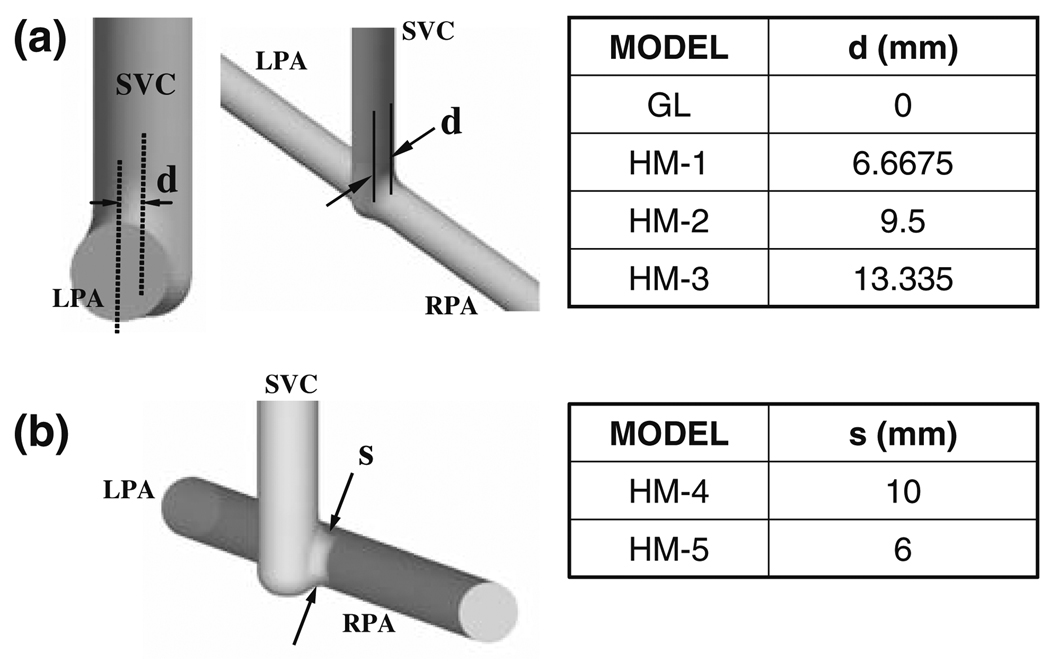
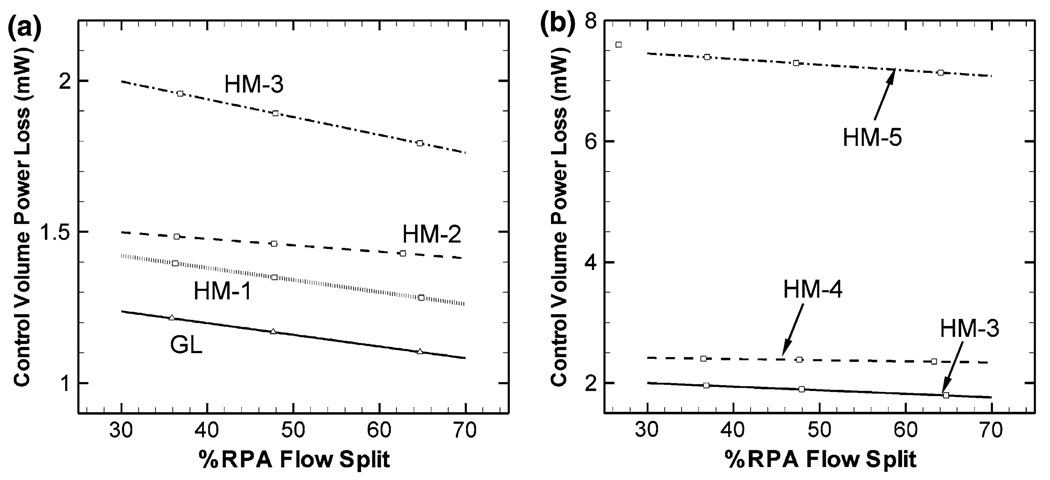
Flow structures, hemodynamics and the hydrodynamic surgical pathway resistances of the final stage functional single ventricle reconstruction, namely the total cavopulmonary connection (TCPC) anatomy, have been investigated extensively. However, the second stage surgical anatomy (i.e., bi-directional Glenn or hemi-Fontan template) has received little attention. We thus initiated a multi-faceted study, involving magnetic resonance imaging (MRI), phase contrast MRI, computational and experimental fluid dynamics methodologies, focused on the second stage of the procedure. Twenty three-dimensional computer and rapid prototype models of 2nd stage TCPC anatomies were created, including idealized parametric geometries (n = 6), patient-specific anatomies (n = 7), and their virtual surgery variant (n = 7). Results in patient-specific and idealized models showed that the Glenn connection template is hemodynamically more efficient with (83% p = 0.08 in patient-specific models and 66% in idealized models) lower power losses compared to hemi-Fontan template, respectively, due to its direct end-to-side anastomosis. Among the several secondary surgical geometrical features, stenosis at the SVC anastomosis or in pulmonary branches was found to be the most critical parameter in increasing the power loss. The pouch size and flare shape were found to be less significant. Compared to the third stage surgery the hydrodynamic resistance of the 2nd stage is considerably lower (both in idealized models and in anatomical models at MRI resting conditions) for both hemi- and Glenn templates. These results can impact the surgical design and planning of the staged TCPC reconstruction.
终末期功能性单心室重建(即全腔静脉肺动脉连接术,TCPC)的血流结构、血流动力学及流体动力手术路径阻力已得到广泛研究。然而,二期手术解剖结构(即双向格林或半Fontan模板)却很少受到关注。因此,我们启动了一项多方面的研究,涉及磁共振成像(MRI)、相位对比MRI、计算流体动力学和实验流体动力学方法,重点关注该手术的第二阶段。创建了23个二维计算机模型和快速原型模型,用于模拟二期TCPC解剖结构,包括理想化参数几何模型(n = 6)、患者特异性解剖模型(n = 7)及其虚拟手术变体模型(n = 7)。患者特异性模型和理想化模型的结果显示,由于格林连接模板采用直接端侧吻合,其血流动力学效率更高(患者特异性模型中为83%,p = 0.08;理想化模型中为66%),与半Fontan模板相比,功率损失更低。在几个次要手术几何特征中,上腔静脉吻合处或肺分支处的狭窄被发现是增加功率损失的最关键参数。袋状大小和喇叭形状的影响较小。与三期手术相比,半Fontan模板和格林模板在二期手术时的流体动力阻力(在MRI静息状态下的理想化模型和解剖模型中)均显著更低。这些结果可能会影响分期TCPC重建的手术设计和规划。