Rothman Jason, Egleston Brian, Wong Yu-Ning, Iffrig Kevan, Lebovitch Steve, Uzzo Robert G
Department of Urologic Oncology, Fox Chase Cancer Center, Philadelphia, Pennsylvania, USA.
J Urol. 2009 Jan;181(1):29-33; discussion 33-4. doi: 10.1016/j.juro.2008.09.009. Epub 2008 Nov 13.
We determined whether a relationship exists between primary tumor size and histopathological features in cases of localized renal cancer.
SEER data were used to create a cohort of patients who were diagnosed with localized node negative renal masses from 1988 to 2004. Nuclear grade was divided into low and high grade groups. We used a multinomial logistic model to predict the probability of nuclear grade and histological subtype with increasing primary tumor size.
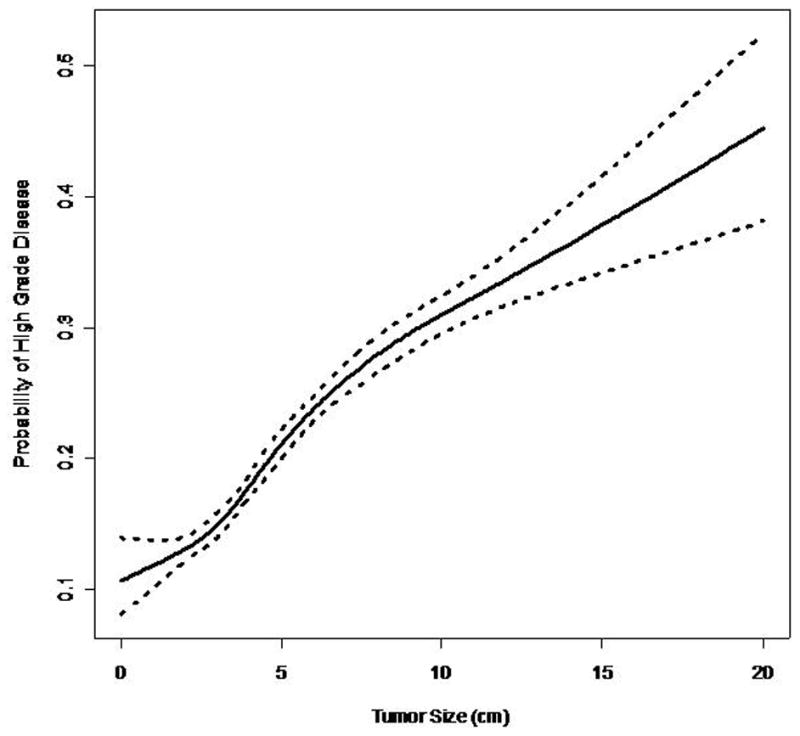
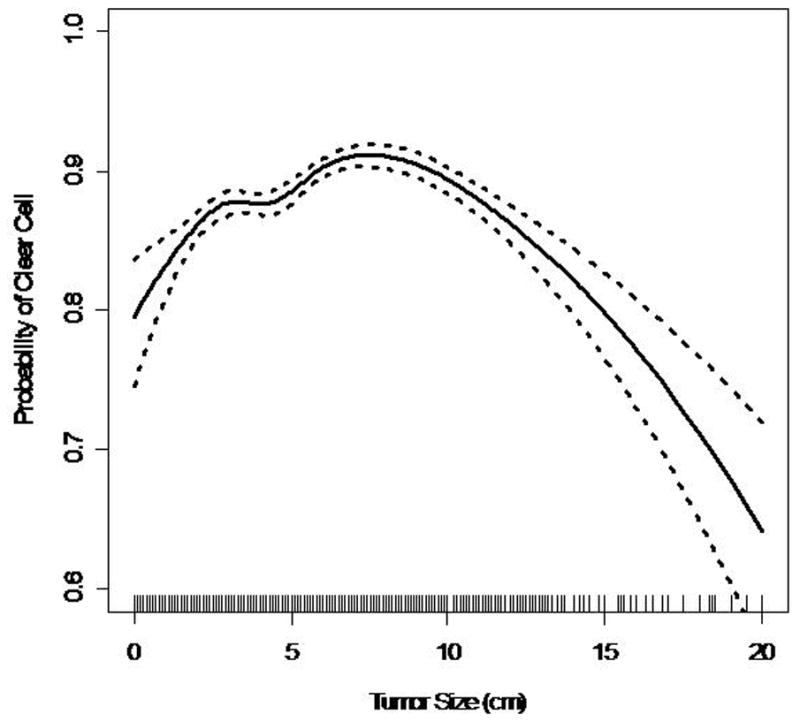
SEER data showed that 19,932 patients with localized renal masses were evaluated. The overall nuclear grade distribution was 80% and 20% for low and high grade tumors, respectively. A multinomial logistic model revealed that the probability of a high grade tumor increased with size. For each 1 cm increase in size of a primary localized renal cell carcinoma the odds of high grade disease increased by 13% (OR 1.13, p <0.001). Multinomial models also predicted that the odds of papillary vs clear cell renal cell carcinoma decreased with tumor size. Conversely the odds of chromophobe vs clear cell renal cell carcinoma increased with increasing tumor size.
Most localized node negative renal cell carcinomas are low grade. Although the probability of a high grade tumor increases with size, almost 85% of renal cell carcinomas smaller than 4 cm and 70% of localized renal cell carcinomas larger than 7 cm demonstrate low nuclear grade. The probability of detecting particular histological subtypes also varies with increasing tumor size. These data suggest that many localized renal tumors can grow large locally without acquiring metastatic potential.
我们确定了局限性肾癌病例中,原发肿瘤大小与组织病理学特征之间是否存在关联。
利用监测、流行病学与最终结果(SEER)数据库的数据,建立了一个队列,纳入1988年至2004年期间被诊断为局限性淋巴结阴性肾肿块的患者。核分级分为低级别组和高级别组。我们使用多项逻辑模型来预测随着原发肿瘤大小增加,核分级和组织学亚型的概率。
SEER数据显示,对19932例局限性肾肿块患者进行了评估。低级别和高级别肿瘤的总体核分级分布分别为80%和20%。多项逻辑模型显示,高级别肿瘤的概率随肿瘤大小增加而升高。对于原发性局限性肾细胞癌,肿瘤大小每增加1 cm,高级别疾病的几率增加13%(比值比1.13,p<0.001)。多项模型还预测,乳头状肾细胞癌与透明细胞肾细胞癌相比的几率随肿瘤大小降低。相反,嫌色细胞肾细胞癌与透明细胞肾细胞癌相比的几率随肿瘤大小增加而升高。
大多数局限性淋巴结阴性肾细胞癌为低级别。尽管高级别肿瘤的概率随肿瘤大小增加而升高,但几乎85%直径小于4 cm的肾细胞癌和70%直径大于7 cm的局限性肾细胞癌显示为低核分级。检测特定组织学亚型的概率也随肿瘤大小增加而变化。这些数据表明,许多局限性肾肿瘤可在局部生长至较大体积而不具备转移潜能。