Wang Yaoming, Thiyagarajan Meenakshisundaram, Chow Nienwen, Singh Itender, Guo Huang, Davis Thomas P, Zlokovic Berislav V
Department for Neurosurgery, Center for Neurodegenerative and Vascular Brain Disorders, University of Rochester Medical Center, Rochester, NY 14642, USA.
Stroke. 2009 May;40(5):1864-9. doi: 10.1161/STROKEAHA.108.536680. Epub 2008 Dec 4.
Activated protein C (APC), a protease with anticoagulant and cytoprotective activities, protects neurons and endothelium from ischemic injury. Drotrecogin-alfa activated, a hyperanticoagulant form of human recombinant APC, is currently being studied in patients with ischemic stroke. How changes in APC anticoagulant activity influence APC's neuroprotection and risk for bleeding is not clear.
We used neuronal and brain endothelial cell injury models and middle cerebral artery occlusion in mice to compare efficacy and safety of drotrecogin-alfa activated and human 3K3A-APC, an APC nonanticoagulant mutant.
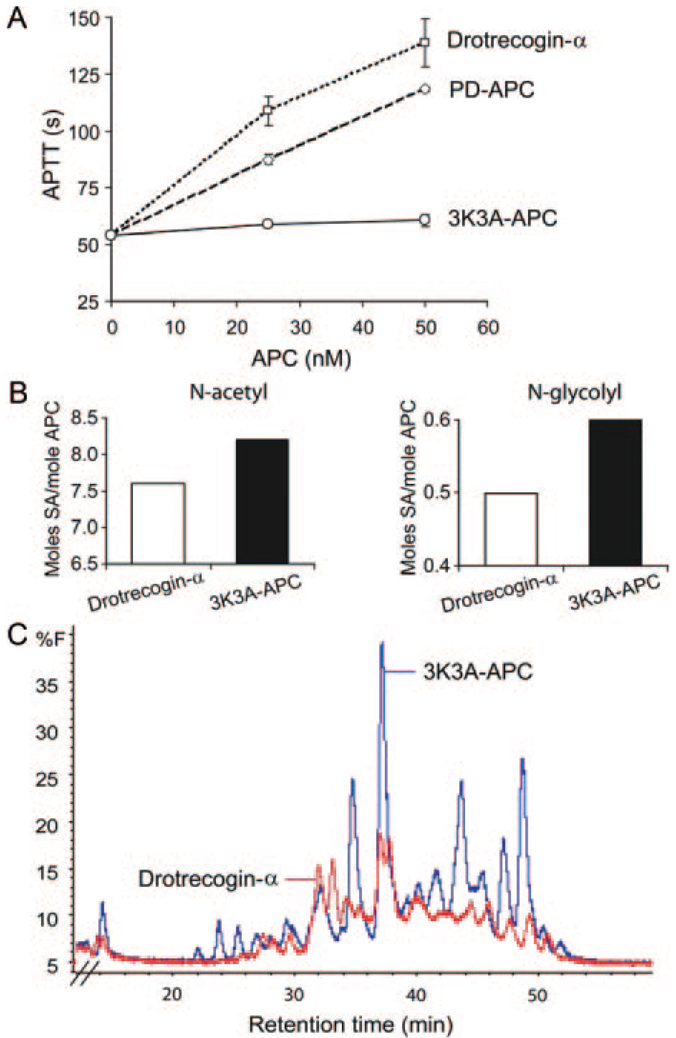
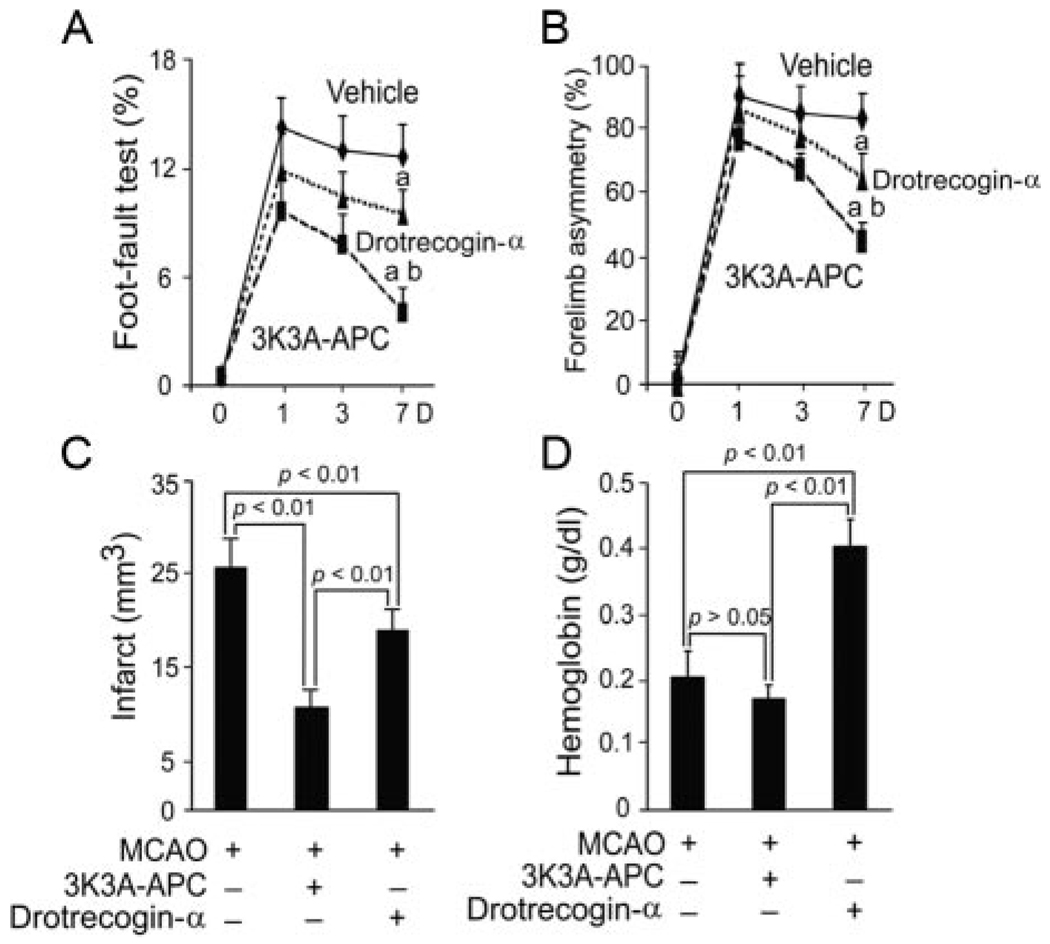
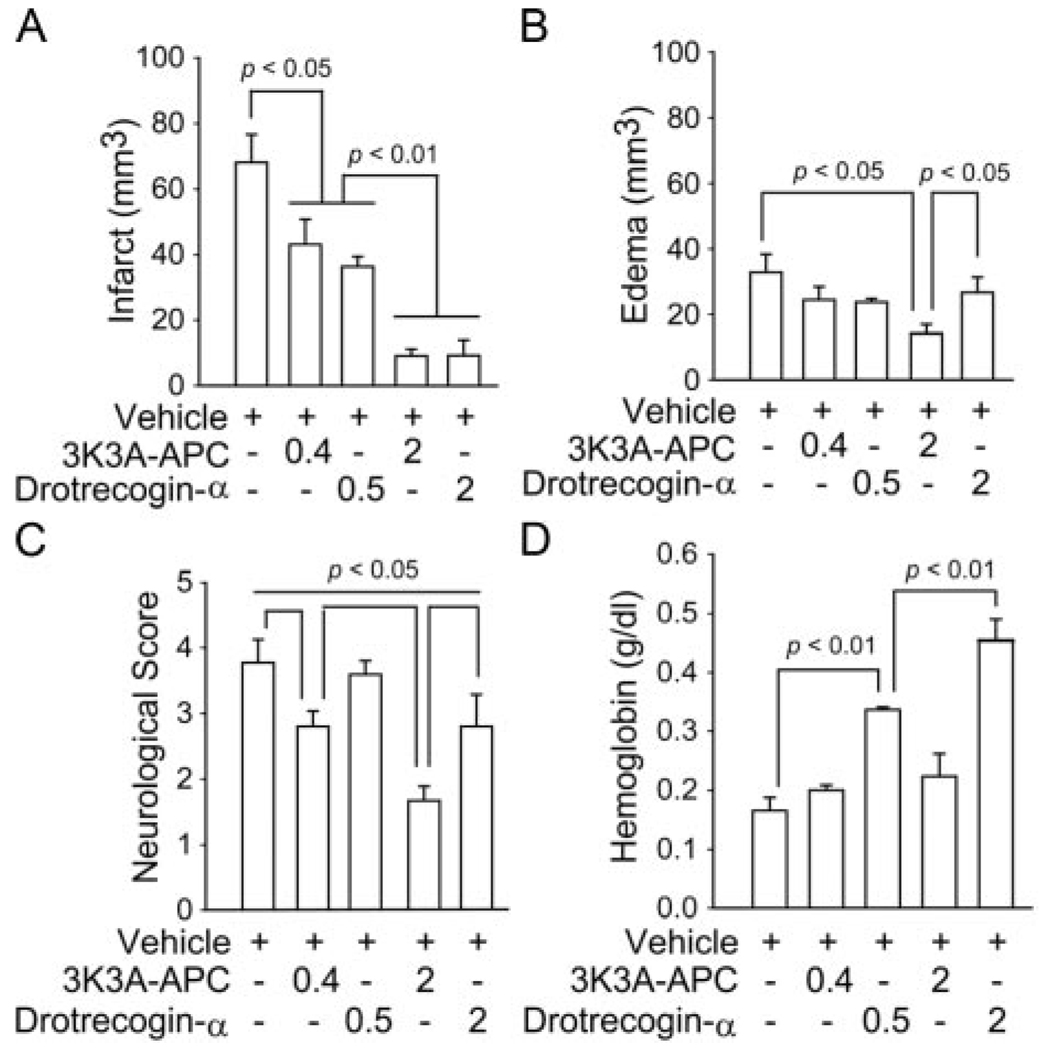
Drotrecogin-alfa activated and 3K3A-APC exhibited 148% and 10% of plasma-derived APC's anticoagulant activity and differ in the carbohydrate content. 3K3A-APC protected mouse neurons from N-methyl-d-aspartate-induced apoptosis and human brain endothelial cell from oxygen-glucose deprivation with 1.8- and 3.1-fold greater efficacy than drotrecogin-alfa activated. Given 5 minutes before transient middle cerebral artery occlusion, 3K3A-APC and drotrecogin-alfa activated (0.5 and 2 mg/kg intravenously) reduced comparably and dose-dependently the infarction lesion up to 85%. 3K3A-APC, but not drotrecogin-alfa activated, improved neurological score dose-dependently (P<0.05). 3K3A-APC did not cause bleeding. In contrast, drotrecogin-alfa activated dose-dependently increased hemoglobin content in postischemic brain. After permanent middle cerebral artery occlusion, 3K3A-APC multidose therapy (1 mg/kg intravenously at 12 hours and 1, 3, 5, and 7 days) improved functional recovery and reduced infarction by 60% with no risk for bleeding, whereas drotrecogin-alfa activated increased hemoglobin deposition in the postischemic brain and showed relatively modest neuroprotection.
Nonanticoagulant 3K3A-APC exhibits greater neuroprotective efficacy with no risk for bleeding compared with drotrecogin-alfa activated, a hyperanticoagulant form of APC.
活化蛋白C(APC)是一种具有抗凝和细胞保护活性的蛋白酶,可保护神经元和内皮细胞免受缺血性损伤。重组人活化蛋白C(drotrecogin - alfa activated)是一种高抗凝形式的人重组APC,目前正在缺血性中风患者中进行研究。APC抗凝活性的变化如何影响其神经保护作用和出血风险尚不清楚。
我们使用神经元和脑内皮细胞损伤模型以及小鼠大脑中动脉闭塞模型,比较重组人活化蛋白C(drotrecogin - alfa activated)和人3K3A - APC(一种APC非抗凝突变体)的疗效和安全性。
重组人活化蛋白C(drotrecogin - alfa activated)和3K3A - APC分别表现出血浆来源APC抗凝活性的148%和10%,且碳水化合物含量不同。3K3A - APC保护小鼠神经元免受N - 甲基 - D - 天冬氨酸诱导的凋亡,并保护人脑内皮细胞免受氧 - 葡萄糖剥夺,其疗效分别比重组人活化蛋白C(drotrecogin - alfa activated)高1.8倍和3.1倍。在短暂性大脑中动脉闭塞前5分钟给予,3K3A - APC和重组人活化蛋白C(drotrecogin - alfa activated,静脉注射0.5和2 mg/kg)同等程度且剂量依赖性地减少梗死灶达85%。3K3A - APC可剂量依赖性地改善神经功能评分(P<0.05),而重组人活化蛋白C(drotrecogin - alfa activated)则不能。3K3A - APC不会引起出血。相比之下,重组人活化蛋白C(drotrecogin - alfa activated)可剂量依赖性地增加缺血后脑中的血红蛋白含量。在永久性大脑中动脉闭塞后,3K3A - APC多剂量治疗(在12小时以及第1、3、5和7天静脉注射1 mg/kg)可改善功能恢复并减少60%的梗死灶,且无出血风险,而重组人活化蛋白C(drotrecogin - alfa activated)增加了缺血后脑中的血红蛋白沉积,且神经保护作用相对较弱。
与高抗凝形式的APC即重组人活化蛋白C(drotrecogin - alfa activated)相比,非抗凝的3K3A - APC具有更强的神经保护作用且无出血风险。