Pasarica Magdalena, Sereda Olga R, Redman Leanne M, Albarado Diana C, Hymel David T, Roan Laura E, Rood Jennifer C, Burk David H, Smith Steven R
Pennington Biomedical Research Center, Baton Rouge, Louisiana, USA.
Diabetes. 2009 Mar;58(3):718-25. doi: 10.2337/db08-1098. Epub 2008 Dec 15.
Based on rodent studies, we examined the hypothesis that increased adipose tissue (AT) mass in obesity without an adequate support of vascularization might lead to hypoxia, macrophage infiltration, and inflammation.
Oxygen partial pressure (AT pO2) and AT temperature in abdominal AT (9 lean and 12 overweight/obese men and women) was measured by direct insertion of a polarographic Clark electrode. Body composition was measured by dual-energy X-ray absorptiometry, and insulin sensitivity was measured by hyperinsulinemic-euglycemic clamp. Abdominal subcutaneous tissue was used for staining, quantitative RT-PCR, and chemokine secretion assay.
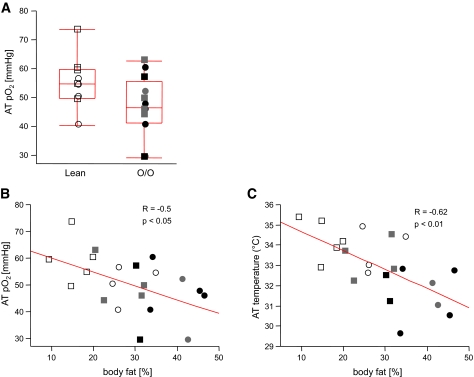
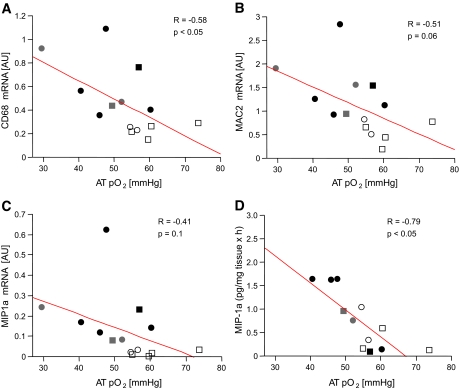
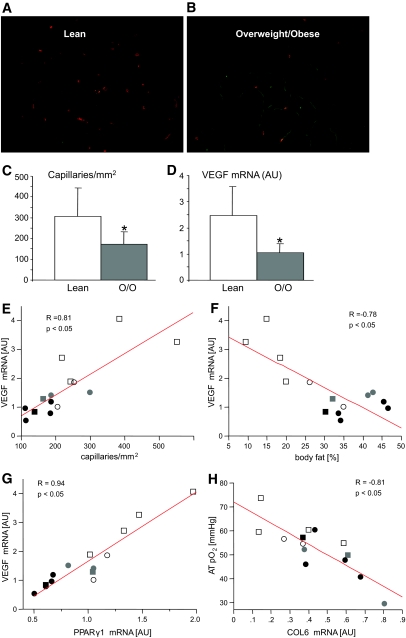
AT pO2 was lower in overweight/obese subjects than lean subjects (47 +/- 10.6 vs. 55 +/- 9.1 mmHg); however, this level of pO2 did not activate the classic hypoxia targets (pyruvate dehydrogenase kinase and vascular endothelial growth factor [VEGF]). AT pO2 was negatively correlated with percent body fat (R = -0.50, P < 0.05). Compared with lean subjects, overweight/obese subjects had 44% lower capillary density and 58% lower VEGF, suggesting AT rarefaction (capillary drop out). This might be due to lower peroxisome proliferator-activated receptor gamma1 and higher collagen VI mRNA expression, which correlated with AT pO2 (P < 0.05). Of clinical importance, AT pO2 negatively correlated with CD68 mRNA and macrophage inflammatory protein 1alpha secretion (R = -0.58, R = -0.79, P < 0.05), suggesting that lower AT pO2 could drive AT inflammation in obesity.
Adipose tissue rarefaction might lie upstream of both low AT pO2 and inflammation in obesity. These results suggest novel approaches to treat the dysfunctional AT found in obesity.
基于啮齿动物研究,我们检验了如下假设:肥胖状态下脂肪组织(AT)质量增加,但缺乏足够的血管化支持,可能导致缺氧、巨噬细胞浸润和炎症。
通过直接插入极谱型克拉克电极,测量了腹部AT(9名瘦人和12名超重/肥胖男性及女性)中的氧分压(AT pO2)和AT温度。通过双能X线吸收法测量身体成分,通过高胰岛素-正葡萄糖钳夹技术测量胰岛素敏感性。腹部皮下组织用于染色、定量逆转录聚合酶链反应(RT-PCR)和趋化因子分泌测定。
超重/肥胖受试者的AT pO2低于瘦人(47±10.6对55±9.1 mmHg);然而,该pO2水平并未激活经典的缺氧靶点(丙酮酸脱氢酶激酶和血管内皮生长因子[VEGF])。AT pO2与体脂百分比呈负相关(R = -0.50,P < 0.05)。与瘦人相比,超重/肥胖受试者的毛细血管密度低44%,VEGF低58%,提示AT稀疏(毛细血管缺失)。这可能是由于过氧化物酶体增殖物激活受体γ1较低和胶原蛋白VI mRNA表达较高,这与AT pO2相关(P < 0.05)。具有临床重要性的是,AT pO2与CD68 mRNA和巨噬细胞炎性蛋白1α分泌呈负相关(R = -0.58,R = -0.79,P < 0.05),提示较低的AT pO2可能在肥胖中驱动AT炎症。
脂肪组织稀疏可能处于肥胖中低AT pO2和炎症的上游。这些结果提示了治疗肥胖中功能失调的AT的新方法。