Eyre R, Feltbower R G, Mubwandarikwa E, Jenkinson H C, Parkes S, Birch J M, Eden T O B, James P W, McKinney P A, Pearce M S, McNally R J Q
Institute of Health and Society, Newcastle University, Newcastle upon Tyne NE1 4LP, UK.
Br J Cancer. 2009 Jan 13;100(1):188-93. doi: 10.1038/sj.bjc.6604837.
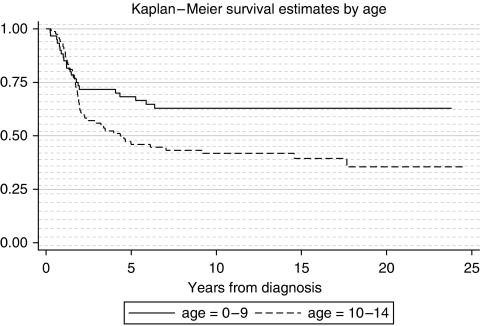
There is a paucity of population-based studies examining incidence and survival trends in childhood bone tumours. We used high quality data from four population-based registries in England. Incidence patterns and trends were described using Poisson regression. Survival trends were analysed using Cox regression. There were 374 cases of childhood (ages 0-14 years) bone tumours (206 osteosarcomas, 144 Ewing sarcomas, 16 chondrosarcomas, 8 other bone tumours) registered in the period 1981-2002. Overall incidence (per million person years) rates were 2.63 (95% confidence interval (CI) 2.27-2.99) for osteosarcoma, 1.90 (1.58-2.21) for Ewing sarcoma and 0.21 (0.11-0.31) for chondrosarcoma. Incidence of Ewing sarcoma declined at an average rate of 3.1% (95% CI 0.6-5.6) per annum (P=0.04), which may be due to tumour reclassification, but there was no change in osteosarcoma incidence. Survival showed marked improvement over the 20 years (1981-2000) for Ewing sarcoma (hazard ratio (HR) per annum=0.95 95% CI 0.91-0.99; P=0.02). However, no improvement was seen for osteosarcoma patients (HR per annum=1.02 95% CI 0.98-1.05; P=0.35) over this time period. Reasons for failure to improve survival including potential delays in diagnosis, accrual to trials, adherence to therapy and lack of improvement in treatment strategies all need to be considered.
关于儿童骨肿瘤发病率和生存趋势的基于人群的研究较少。我们使用了来自英格兰四个基于人群的登记处的高质量数据。发病率模式和趋势采用泊松回归进行描述。生存趋势采用Cox回归进行分析。1981年至2002年期间登记了374例儿童(0至14岁)骨肿瘤病例(206例骨肉瘤、144例尤因肉瘤、16例软骨肉瘤、8例其他骨肿瘤)。骨肉瘤的总体发病率(每百万人口年)为2.63(95%置信区间(CI)2.27 - 2.99),尤因肉瘤为1.90(1.58 - 2.21),软骨肉瘤为0.21(0.11 - 0.31)。尤因肉瘤的发病率以每年平均3.1%(95%CI 0.6 - 5.6)的速度下降(P = 0.04),这可能是由于肿瘤重新分类,但骨肉瘤发病率没有变化。在1981年至2000年的20年中,尤因肉瘤的生存率有显著提高(每年风险比(HR)= 0.95,95%CI 0.91 - 0.99;P = 0.02)。然而,在此期间骨肉瘤患者的生存率没有改善(每年HR = 1.02,95%CI 0.98 - 1.05;P = 0.35)。未能提高生存率的原因包括诊断可能的延迟、参加试验、坚持治疗以及治疗策略缺乏改进等,所有这些都需要考虑。