Tsapenko Mykola V, Tsapenko Arseniy V, Comfere Thomas Bo, Mour Girish K, Mankad Sunil V, Gajic Ognjen
Division of Pulmonary and Critical Care Medicine, Mayo Epidemiology and Translational Research in Intensive Care, Mayo Clinic, Rochester, MN 55905, USA.
Vasc Health Risk Manag. 2008;4(5):1043-60. doi: 10.2147/vhrm.s3998.
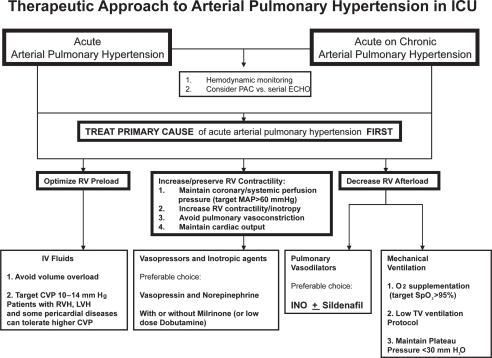
Pulmonary artery pressure elevation complicates the course of many complex disorders treated in a noncardiac intensive care unit. Acute pulmonary hypertension, however, remains underdiagnosed and its treatment frequently begins only after serious complications have developed. Significant pathophysiologic differences between acute and chronic pulmonary hypertension make current classification and treatment recommendations for chronic pulmonary hypertension barely applicable to acute pulmonary hypertension. In order to clarify the terminology of acute pulmonary hypertension and distinguish it from chronic pulmonary hypertension, we provide a classification of acute pulmonary hypertension according to underlying pathophysiologic mechanisms, clinical features, natural history, and response to treatment. Based on available data, therapy of acute arterial pulmonary hypertension should generally be aimed at acutely relieving right ventricular (RV) pressure overload and preventing RV dysfunction. Cases of severe acute pulmonary hypertension complicated by RV failure and systemic arterial hypotension are real clinical challenges requiring tight hemodynamic monitoring and aggressive treatment including combinations of pulmonary vasodilators, inotropic agents and systemic arterial vasoconstrictors. The choice of vasopressor and inotropes in patients with acute pulmonary hypertension should take into consideration their effects on vascular resistance and cardiac output when used alone or in combinations with other agents, and must be individualized based on patient response.
肺动脉压力升高使许多在非心脏重症监护病房治疗的复杂疾病的病程复杂化。然而,急性肺动脉高压仍然诊断不足,其治疗通常仅在出现严重并发症后才开始。急性和慢性肺动脉高压之间存在显著的病理生理差异,使得目前针对慢性肺动脉高压的分类和治疗建议几乎不适用于急性肺动脉高压。为了明确急性肺动脉高压的术语并将其与慢性肺动脉高压区分开来,我们根据潜在的病理生理机制、临床特征、自然病史和治疗反应对急性肺动脉高压进行了分类。根据现有数据,急性动脉性肺动脉高压的治疗通常应旨在急性缓解右心室(RV)压力过载并预防RV功能障碍。严重急性肺动脉高压合并RV衰竭和体循环动脉低血压的病例是真正的临床挑战,需要严密的血流动力学监测和积极治疗,包括联合使用肺血管扩张剂、正性肌力药物和体循环动脉血管收缩剂。急性肺动脉高压患者血管升压药和正性肌力药物的选择应考虑其单独使用或与其他药物联合使用时对血管阻力和心输出量的影响,并且必须根据患者反应进行个体化选择。