Huicho Luis, Trelles Miguel, Gonzales Fernando, Mendoza Walter, Miranda Jaime
Department of Paediatrics, Universidad Nacional Mayor de San Marcos, Lima, Peru.
BMC Public Health. 2009 Feb 2;9:47. doi: 10.1186/1471-2458-9-47.
Sub-national analyses of causes of death and time-trends help to define public health policy priorities. They are particularly important in countries undergoing epidemiological transition like Peru. There are no studies exploring Peruvian national and regional characteristics of such epidemiological transition. We aimed to describe Peru's national and regional mortality profiles between 1996 and 2000.
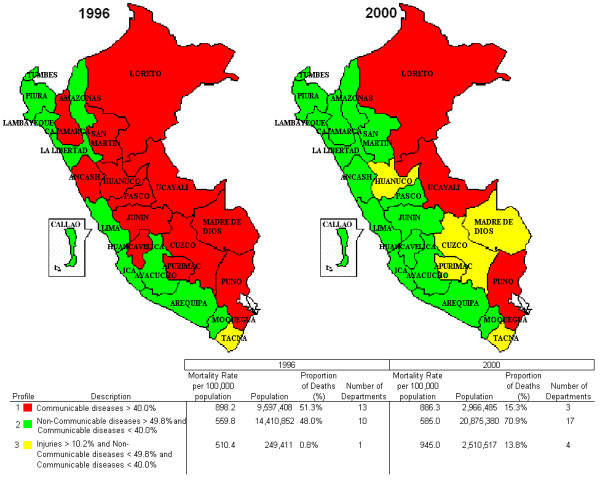
Registered mortality data for the study period were corrected for under-registration following standardized methods. Main causes of death by age group and by geographical region were determined. Departmental mortality profiles were constructed to evaluate mortality transition, using 1996 data as baseline. Annual cumulative slopes for the period 1996-2000 were estimated for each department and region.
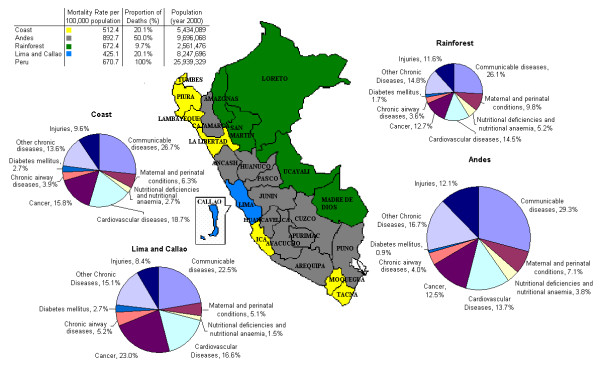
For the study period non-communicable diseases explained more than half of all causes of death, communicable diseases more than one third, and injuries 10.8% of all deaths. Lima accounted for 32% of total population and 20% of total deaths. The Andean region, with 38% of Peru's population, accounted for half of all country deaths. Departmental mortality predominance shifted from communicable diseases in 1996 towards non-communicable diseases and injuries in 2000. Maternal and perinatal conditions, and nutritional deficiencies and nutritional anaemia declined markedly in all departments and regions. Infectious diseases decreased in all regions except Lima. In all regions acute respiratory infections are a leading cause of death, but their proportion ranged from 9.3% in Lima and Callao to 15.3% in the Andean region. Tuberculosis and injuries ranked high in Lima and the Andean region.
Peruvian mortality shows a double burden of communicable and non-communicable, with increasing importance of non-communicable diseases and injuries. This challenges national and sub-national health system performance and policy making.
对死因和时间趋势进行次国家级分析有助于确定公共卫生政策重点。在像秘鲁这样正在经历流行病学转变的国家,这些分析尤为重要。目前尚无研究探讨秘鲁这种流行病学转变的国家和地区特征。我们旨在描述1996年至2000年期间秘鲁的国家和地区死亡率概况。
按照标准化方法对研究期间登记的死亡数据进行漏报校正。确定按年龄组和地理区域划分的主要死因。以1996年数据为基线,构建各部门死亡率概况以评估死亡率转变。估算了1996 - 2000年期间每个部门和地区的年度累积斜率。
在研究期间,非传染性疾病占所有死因的一半以上,传染病占三分之一以上,伤害占所有死亡的10.8%。利马占总人口的32%,占总死亡人数的20%。占秘鲁人口38%的安第斯地区占全国死亡人数的一半。各部门死亡率优势从1996年的传染病转向2000年的非传染性疾病和伤害。所有部门和地区的孕产妇和围产期疾病、营养缺乏和营养性贫血显著下降。除利马外,所有地区的传染病均有所减少。在所有地区,急性呼吸道感染都是主要死因,但其比例在利马和卡亚俄为9.3%,在安第斯地区为15.3%。结核病和伤害在利马和安第斯地区排名靠前。
秘鲁的死亡率呈现出传染病和非传染病的双重负担,非传染性疾病和伤害的重要性日益增加。这对国家和次国家级卫生系统的绩效及政策制定构成了挑战。