Burke Wylie, Culver Julie, Pinsky Linda, Hall Sarah, Reynolds Susan E, Yasui Yutaka, Press Nancy
Department of Bioethics and Humanities, University of Washington, Seattle, Washington 98195-7120, USA.
Am J Med Genet A. 2009 Mar;149A(3):349-56. doi: 10.1002/ajmg.a.32643.
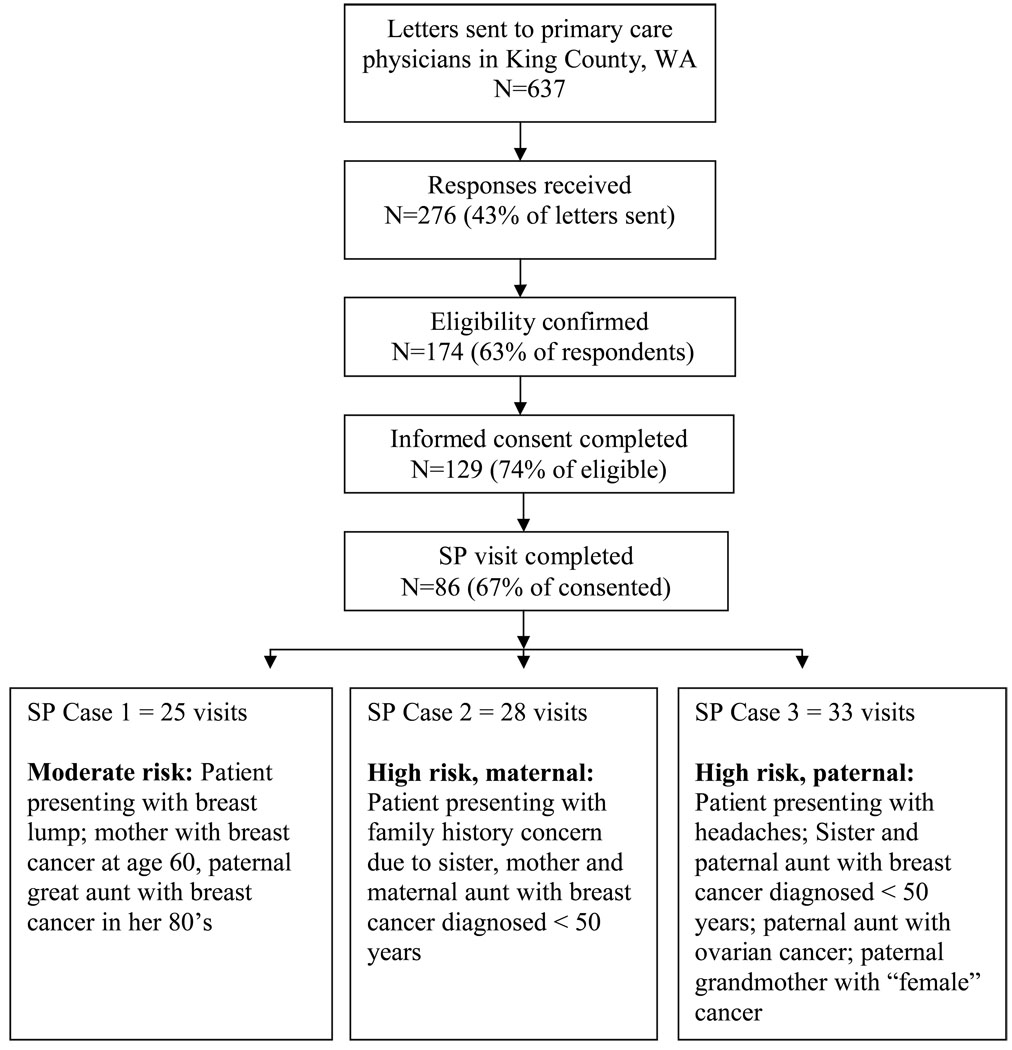
Family history is increasingly important in primary care as a means to detect candidates for genetic testing or tailored prevention programs. We evaluated primary care physicians' skills in assessing family history for breast cancer risk, using unannounced standardized patient (SP) visits to 86 general internists and family medicine practitioners in King County, WA. Transcripts of clinical encounters were coded to determine ascertainment of family history, risk assessment, and clinical follow-up. Physicians in our study collected sufficient family history to assess breast cancer risk in 48% of encounters with an anxious patient at moderate risk, 100% of encounters with a patient who had a strong maternal family history of breast cancer, and 45% of encounters with a patient who had a strong paternal family history of breast and ovarian cancer. Increased risk was usually communicated in terms of recommendations for preventive action. Few physicians referred patients to genetic counseling, few associated ovarian cancer with breast cancer risk, and some incorrectly discounted paternal family history of breast cancer. We conclude that pedigree assessment of breast cancer risk is feasible in primary care, but may occur consistently only when a strong maternal family history is present. Primary care education should focus on the link between inherited breast and ovarian cancer risk and on the significance of paternal family history. Educational efforts may be most successful when they emphasize the value of genetic counseling for individuals at risk for inherited cancer and the connection between genetic risk and specific prevention measures.
家族史在初级保健中作为检测基因检测候选者或量身定制预防方案的一种手段正变得越来越重要。我们通过对华盛顿州金县86名普通内科医生和家庭医生进行未事先通知的标准化患者(SP)访视,评估了初级保健医生评估乳腺癌风险家族史的技能。对临床诊疗记录进行编码,以确定家族史的确定情况、风险评估和临床随访情况。在我们的研究中,医生在48%与中度风险焦虑患者的诊疗中、100%与有强烈乳腺癌母系家族史患者的诊疗中以及45%与有强烈乳腺癌和卵巢癌父系家族史患者的诊疗中,收集了足够的家族史来评估乳腺癌风险。增加的风险通常以预防行动建议的形式传达。很少有医生将患者转介进行遗传咨询,很少有人将卵巢癌与乳腺癌风险联系起来,还有一些人错误地忽视了父系家族的乳腺癌病史。我们得出结论,在初级保健中对乳腺癌风险进行系谱评估是可行的,但可能只有在存在强烈的母系家族史时才会持续进行。初级保健教育应侧重于遗传性乳腺癌和卵巢癌风险之间的联系以及父系家族史的重要性。当强调对遗传性癌症风险个体进行遗传咨询的价值以及遗传风险与特定预防措施之间的联系时,教育努力可能最为成功。