Dixon Sherry L, Gaitens Joanna M, Jacobs David E, Strauss Warren, Nagaraja Jyothi, Pivetz Tim, Wilson Jonathan W, Ashley Peter J
National Center for Healthy Housing, Columbia, Maryland 21044, USA.
Environ Health Perspect. 2009 Mar;117(3):468-74. doi: 10.1289/ehp.11918. Epub 2008 Nov 14.
The U.S. Centers for Disease Control and Prevention collected health, housing, and environmental data in a single integrated national survey for the first time in the United States in 1999-2004.
We aimed to determine how floor dust lead (PbD) loadings and other housing factors influence childhood blood lead (PbB) levels and lead poisoning.
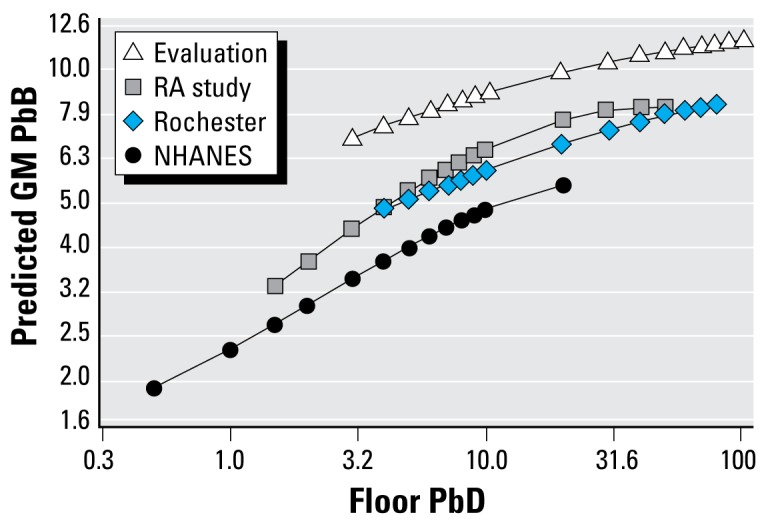
We analyzed data from the 1999-2004 National Health and Nutrition Examination Survey (NHANES), including 2,155 children 12-60 months of age with PbB and PbD measurements. We used linear and logistic regression models to predict log-transformed PbB and the odds that PbB was >or=5 and >or=10 microg/dL at a range of floor PbD.
The population-weighted geometric mean (GM) PbB was 2.0 microg/dL (geometric standard error=1.0). Age of child, race/ethnicity, serum cotinine concentration, poverty-to-income ratio, country of birth, year of building construction, floor PbD by floor surface and condition, windowsill PbD, presence of deteriorated paint, home-apartment type, smoking in the home, and recent renovation were significant predictors in either the linear model [the proportion of variability in the dependent variable accounted for by the model (R2)=40%] or logistic model for 10 microg/dL (R2=5%). At floor PbD=12 microg/ft2, the models predict that 4.6% of children living in homes constructed before 1978 have PbB>or=10 microg/dL, 27% have PbB>or=5 microg/dL, and the GM PbB is 3.9 microg/dL.
Lowering the floor PbD standard below the current standard of 40 microg/ft2 would protect more children from elevated PbB.
1999 - 2004年,美国疾病控制与预防中心首次在美国一项综合全国调查中收集了健康、住房和环境数据。
我们旨在确定地板灰尘铅(PbD)负荷及其他住房因素如何影响儿童血铅(PbB)水平和铅中毒情况。
我们分析了1999 - 2004年国家健康与营养检查调查(NHANES)的数据,其中包括2155名12至60个月大且有PbB和PbD测量值的儿童。我们使用线性和逻辑回归模型来预测对数转换后的PbB以及在一系列地板PbD水平下PbB大于或等于5微克/分升和大于或等于10微克/分升的几率。
人群加权几何均值(GM)PbB为2.0微克/分升(几何标准误差 = 1.0)。儿童年龄、种族/民族、血清可替宁浓度、贫困与收入比率、出生国家、建筑年份、按地板表面和状况划分的地板PbD、窗台PbD、是否存在油漆剥落、住宅/公寓类型、家中吸烟情况以及近期装修情况,在预测线性模型[模型解释的因变量变异比例(R2)= 40%]或针对10微克/分升的逻辑模型(R2 = 5%)中均为显著预测因素。当地板PbD = 12微克/平方英尺时,模型预测在1978年以前建造的房屋中,4.6%的儿童PbB大于或等于10微克/分升,27%的儿童PbB大于或等于5微克/分升,GM PbB为3.9微克/分升。
将地板PbD标准降至当前40微克/平方英尺的标准以下,可保护更多儿童免受血铅升高的影响。