Jack Clifford R, Lowe Val J, Weigand Stephen D, Wiste Heather J, Senjem Matthew L, Knopman David S, Shiung Maria M, Gunter Jeffrey L, Boeve Bradley F, Kemp Bradley J, Weiner Michael, Petersen Ronald C
Clifford R. Jack, Mayo Clinic, Diagnostic Radiology, 200 First Street SW, Rochester, MN 55905, USA.
Brain. 2009 May;132(Pt 5):1355-65. doi: 10.1093/brain/awp062. Epub 2009 Mar 31.
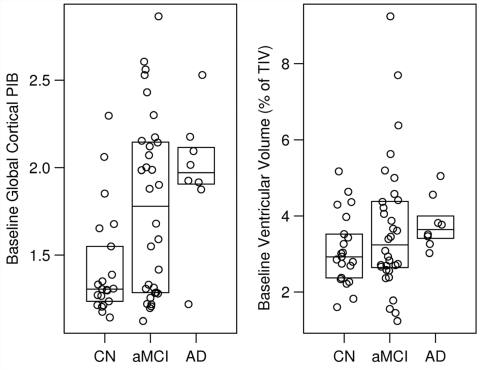
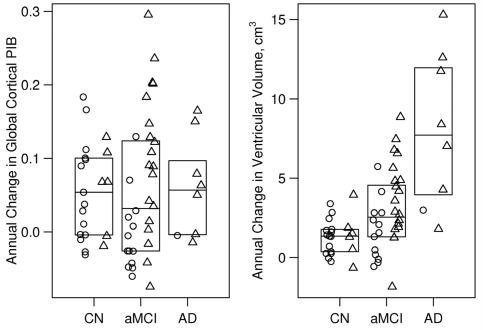
The purpose of this study was to use serial imaging to gain insight into the sequence of pathologic events in Alzheimer's disease, and the clinical features associated with this sequence. We measured change in amyloid deposition over time using serial (11)C Pittsburgh compound B (PIB) positron emission tomography and progression of neurodegeneration using serial structural magnetic resonance imaging. We studied 21 healthy cognitively normal subjects, 32 with amnestic mild cognitive impairment and 8 with Alzheimer's disease. Subjects were drawn from two sources--ongoing longitudinal registries at Mayo Clinic, and the Alzheimer's disease Neuroimaging Initiative (ADNI). All subjects underwent clinical assessments, MRI and PIB studies at two time points, approximately one year apart. PIB retention was quantified in global cortical to cerebellar ratio units and brain atrophy in units of cm(3) by measuring ventricular expansion. The annual change in global PIB retention did not differ by clinical group (P = 0.90), and although small (median 0.042 ratio units/year overall) was greater than zero among all subjects (P < 0.001). Ventricular expansion rates differed by clinical group (P < 0.001) and increased in the following order: cognitively normal (1.3 cm(3)/year) < amnestic mild cognitive impairment (2.5 cm(3)/year) < Alzheimer's disease (7.7 cm(3)/year). Among all subjects there was no correlation between PIB change and concurrent change on CDR-SB (r = -0.01, P = 0.97) but some evidence of a weak correlation with MMSE (r =-0.22, P = 0.09). In contrast, greater rates of ventricular expansion were clearly correlated with worsening concurrent change on CDR-SB (r = 0.42, P < 0.01) and MMSE (r =-0.52, P < 0.01). Our data are consistent with a model of typical late onset Alzheimer's disease that has two main features: (i) dissociation between the rate of amyloid deposition and the rate of neurodegeneration late in life, with amyloid deposition proceeding at a constant slow rate while neurodegeneration accelerates and (ii) clinical symptoms are coupled to neurodegeneration not amyloid deposition. Significant plaque deposition occurs prior to clinical decline. The presence of brain amyloidosis alone is not sufficient to produce cognitive decline, rather, the neurodegenerative component of Alzheimer's disease pathology is the direct substrate of cognitive impairment and the rate of cognitive decline is driven by the rate of neurodegeneration. Neurodegeneration (atrophy on MRI) both precedes and parallels cognitive decline. This model implies a complimentary role for MRI and PIB imaging in Alzheimer's disease, with each reflecting one of the major pathologies, amyloid dysmetabolism and neurodegeneration.
本研究的目的是通过系列成像深入了解阿尔茨海默病病理事件的序列,以及与该序列相关的临床特征。我们使用系列(11)C匹兹堡化合物B(PIB)正电子发射断层扫描测量随时间的淀粉样蛋白沉积变化,并使用系列结构磁共振成像测量神经变性的进展。我们研究了21名认知正常的健康受试者、32名遗忘型轻度认知障碍患者和8名阿尔茨海默病患者。受试者来自两个来源——梅奥诊所正在进行的纵向登记处,以及阿尔茨海默病神经影像倡议(ADNI)。所有受试者在两个时间点接受临床评估、MRI和PIB研究,时间间隔约为一年。通过测量脑室扩张,以整体皮质与小脑的比率单位对PIB保留进行定量,以立方厘米为单位对脑萎缩进行定量。整体PIB保留的年变化在不同临床组之间没有差异(P = 0.90),尽管变化很小(总体中位数为0.042比率单位/年),但在所有受试者中大于零(P < 0.001)。脑室扩张率在不同临床组之间存在差异(P < 0.001),并按以下顺序增加:认知正常(1.3立方厘米/年)<遗忘型轻度认知障碍(2.5立方厘米/年)<阿尔茨海默病(7.7立方厘米/年)。在所有受试者中,PIB变化与CDR-SB的同时变化之间没有相关性(r = -0.01,P = 0.97),但有一些证据表明与MMSE存在弱相关性(r = -0.22,P = 0.09)。相比之下,更高的脑室扩张率与CDR-SB(r = 0.42,P < 0.01)和MMSE(r = -0.52,P < 0.01)的同时恶化变化明显相关。我们的数据与典型晚发型阿尔茨海默病的模型一致,该模型有两个主要特征:(i)生命后期淀粉样蛋白沉积速率与神经变性速率之间的分离,淀粉样蛋白沉积以恒定的缓慢速率进行,而神经变性加速;(ii)临床症状与神经变性而非淀粉样蛋白沉积相关。显著的斑块沉积发生在临床衰退之前。仅脑淀粉样变性的存在不足以导致认知衰退,相反,阿尔茨海默病病理的神经变性成分是认知障碍的直接基础,认知衰退的速率由神经变性的速率驱动。神经变性(MRI上的萎缩)在认知衰退之前出现并与之平行。该模型意味着MRI和PIB成像在阿尔茨海默病中具有互补作用,各自反映主要病理之一,即淀粉样蛋白代谢异常和神经变性。