Mukherjee Sushmita, Wysock James S, Ng Casey K, Akhtar Mohammed, Perner Sven, Lee Ming-Ming, Rubin Mark A, Maxfield Frederick R, Webb Watt W, Scherr Douglas S
Department of Biochemistry, Weill Cornell Medical College, New York, NY.
Proc SPIE Int Soc Opt Eng. 2009;7161. doi: 10.1117/12.808314.
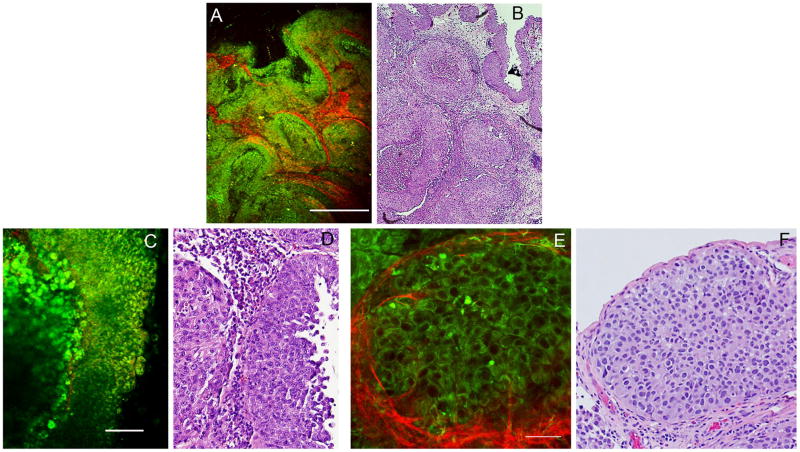
At the time of diagnosis, approximately 75% of bladder cancers are non-muscle invasive. Appropriate diagnosis and surgical resection at this stage improves prognosis dramatically. However, these lesions, being small and/or flat, are often missed by conventional white-light cystoscopes. Furthermore, it is difficult to assess the surgical margin for negativity using conventional cystoscopes. Resultantly, the recurrence rates in patients with early bladder cancer are very high. This is currently addressed by repeat cystoscopies and biopsies, which can last throughout the life of a patient, increasing cost and patient morbidity. Multiphoton endoscopes offer a potential solution, allowing real time, non-invasive biopsies of the human bladder, as well as an up-close assessment of the resection margin. While miniaturization of the Multiphoton microscope into an endoscopic format is currently in progress, we present results here indicating that Multiphoton imaging (using a bench-top Multiphoton microscope) can indeed identify cancers in fresh, unfixed human bladder biopsies. Multiphoton images are acquired in two channels: (1) broadband autofluorescence from cells, and (2) second harmonic generation (SHG), mostly by tissue collagen. These images are then compared with gold standard hematoxylin/eosin (H&E) stained histopathology slides from the same specimen. Based on a "training set" and a very small "blinded set" of samples, we have found excellent correlation between the Multiphoton and histopathological diagnoses. A larger blinded analysis by two independent uropathologists is currently in progress. We expect that the conclusion of this phase will provide us with diagnostic accuracy estimates, as well as the degree of inter-observer heterogeneity.
在诊断时,大约75%的膀胱癌是非肌层浸润性的。在此阶段进行适当的诊断和手术切除可显著改善预后。然而,这些病变小和/或扁平,常被传统白光膀胱镜漏诊。此外,使用传统膀胱镜很难评估手术切缘的阴性情况。因此,早期膀胱癌患者的复发率非常高。目前通过重复膀胱镜检查和活检来解决这一问题,这可能贯穿患者一生,增加了成本和患者的发病率。多光子内窥镜提供了一种潜在的解决方案,能够对人体膀胱进行实时、非侵入性活检,以及对手术切缘进行近距离评估。虽然目前正在将多光子显微镜小型化制成内窥镜形式,但我们在此展示的结果表明,多光子成像(使用台式多光子显微镜)确实可以在新鲜、未固定的人体膀胱活检组织中识别癌症。多光子图像通过两个通道采集:(1)细胞的宽带自发荧光,以及(2)主要由组织胶原蛋白产生的二次谐波生成(SHG)。然后将这些图像与来自同一标本的苏木精/伊红(H&E)染色组织病理学金标准切片进行比较。基于一组“训练集”样本和一个非常小的“盲法集”样本,我们发现多光子诊断与组织病理学诊断之间具有极好的相关性。目前,两位独立的泌尿病理学家正在进行更大规模的盲法分析。我们预计这一阶段的结论将为我们提供诊断准确性估计,以及观察者间异质性的程度。