Ellis Paul, Barrett-Lee Peter, Johnson Lindsay, Cameron David, Wardley Andrew, O'Reilly Susan, Verrill Mark, Smith Ian, Yarnold John, Coleman Robert, Earl Helena, Canney Peter, Twelves Chris, Poole Christopher, Bloomfield David, Hopwood Penelope, Johnston Stephen, Dowsett Mitchell, Bartlett John M S, Ellis Ian, Peckitt Clare, Hall Emma, Bliss Judith M
Guy's and St Thomas' NHS Trust, London, UK.
Lancet. 2009 May 16;373(9676):1681-92. doi: 10.1016/S0140-6736(09)60740-6.
Incorporation of a taxane as adjuvant treatment for early breast cancer offers potential for further improvement of anthracycline-based treatment. The UK TACT study (CRUK01/001) investigated whether sequential docetaxel after anthracycline chemotherapy would improve patient outcome compared with standard chemotherapy of similar duration.
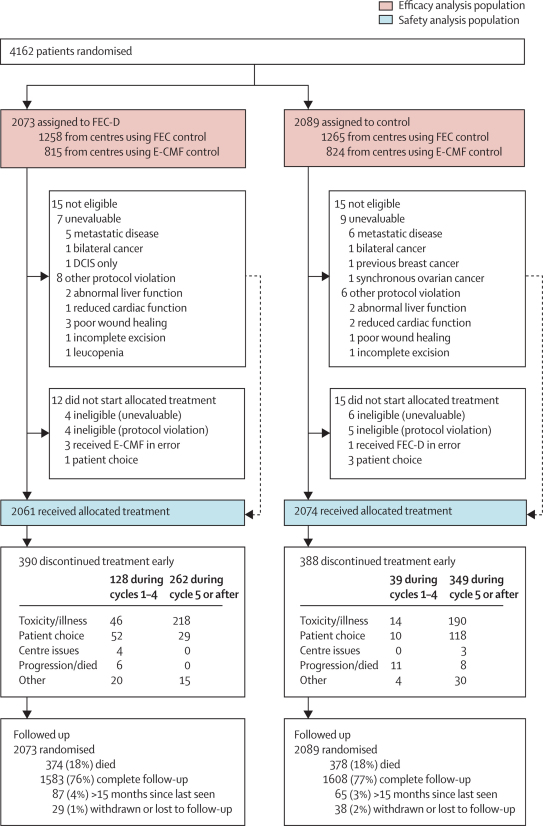
In this multicentre, open-label, phase III, randomised controlled trial, 4162 women (aged >18 years) with node-positive or high-risk node-negative operable early breast cancer were randomly assigned by computer-generated permuted block randomisation to receive FEC (fluorouracil 600 mg/m(2), epirubicin 60 mg/m(2), cyclophosphamide 600 mg/m(2) at 3-weekly intervals) for four cycles followed by docetaxel (100 mg/m(2) at 3-weekly intervals) for four cycles (n=2073) or control (n=2089). For the control regimen, centres chose either FEC for eight cycles (n=1265) or epirubicin (100 mg/m(2) at 3-weekly intervals) for four cycles followed by CMF (cyclophosphamide 600 mg/m(2), methotrexate 40 mg/m(2), and fluorouracil 600 mg/m(2) at 4-weekly intervals) for four cycles (n=824). The primary endpoint was disease-free survival. Analysis was by intention to treat (ITT). This study is registered as an International Standard Randomised Controlled Trial, number ISRCTN79718493.
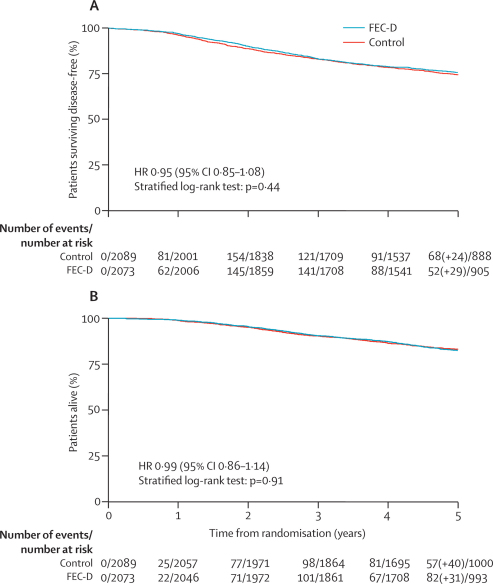
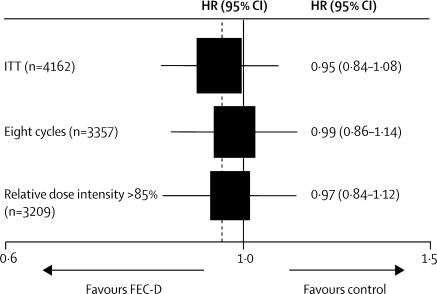
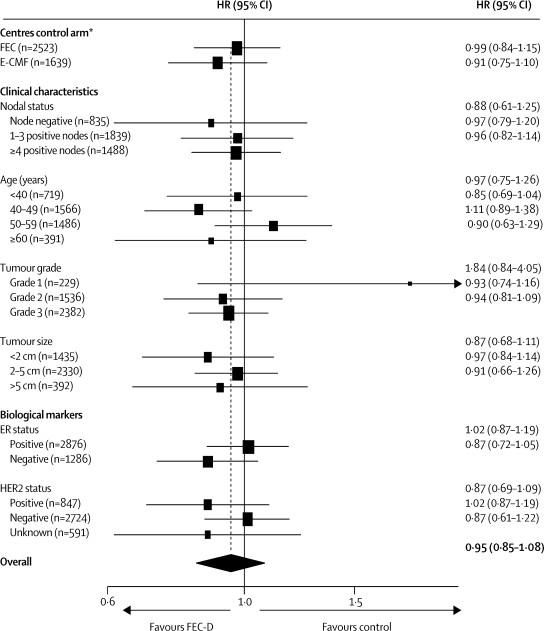
All randomised patients were included in the ITT population. With a median follow-up of 62 months, disease-free survival events were seen in 517 of 2073 patients in the experimental group compared with 539 of 2089 controls (hazard ratio [HR] 0.95, 95% CI 0.85-1.08; p=0.44). 75.6% (95% CI 73.7-77.5) of patients in the experimental group and 74.3% (72.3-76.2) of controls were alive and disease-free at 5 years. The proportion of patients who reported any acute grade 3 or 4 adverse event was significantly greater in the experimental group than in the control group (p<0.0001); the most frequent events were neutropenia (937 events vs 797 events), leucopenia (507 vs 362), and lethargy (456 vs 272).
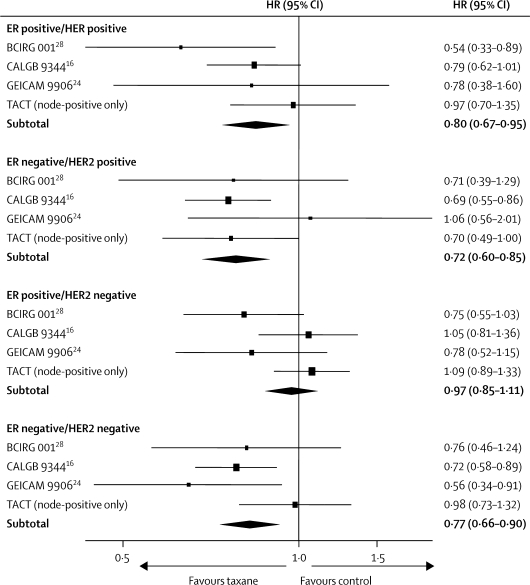
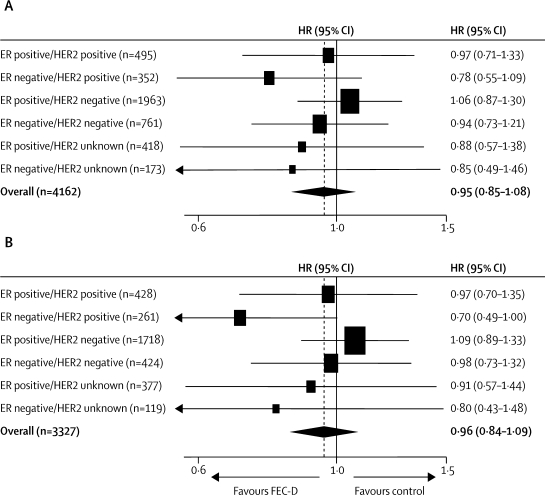
This study did not show any overall gain from the addition of docetaxel to standard anthracycline chemotherapy. Exploration of predictive biomarker-defined subgroups might have the potential to better target the use of taxane-based therapy.
Cancer Research UK (CRUK 01/001), Sanofi-Aventis, Pfizer, and Roche.
将紫杉烷纳入早期乳腺癌的辅助治疗为进一步改善基于蒽环类药物的治疗提供了可能。英国TACT研究(CRUK01/001)调查了与相似疗程的标准化疗相比,蒽环类化疗后序贯多西他赛是否会改善患者预后。
在这项多中心、开放标签、III期随机对照试验中,4162名年龄大于18岁、淋巴结阳性或高危淋巴结阴性的可手术早期乳腺癌女性患者,通过计算机生成的置换区组随机化方法,被随机分配接受FEC方案(氟尿嘧啶600mg/m²、表柔比星60mg/m²、环磷酰胺600mg/m²,每3周一次)共4个周期,随后接受多西他赛(100mg/m²,每3周一次)共4个周期(n = 2073),或对照组治疗(n = 2089)。对于对照方案,各中心选择8个周期的FEC方案(n = 1265),或4个周期的表柔比星(100mg/m²,每3周一次),随后是4个周期的CMF方案(环磷酰胺600mg/m²、甲氨蝶呤40mg/m²、氟尿嘧啶600mg/m²,每4周一次)(n = 824)。主要终点为无病生存期。采用意向性分析(ITT)。本研究已注册为国际标准随机对照试验,编号为ISRCTN79718493。
所有随机分组的患者均纳入ITT人群。中位随访62个月时,试验组2073例患者中有517例出现无病生存事件,而对照组2089例中有539例(风险比[HR]0.95,95%CI 0.85 - 1.08;p = 0.44)。试验组75.6%(95%CI 73.7 - 77.5)的患者和对照组74.3%(72.3 - 76.2)的患者在5年时存活且无病。试验组报告任何3级或4级急性不良事件的患者比例显著高于对照组(p < 0.0001);最常见的事件是中性粒细胞减少(937例事件对797例事件)、白细胞减少(507例对362例)和乏力(456例对272例)。
本研究未显示在标准化蒽环类化疗基础上加用多西他赛有任何总体获益。探索预测性生物标志物定义的亚组可能有潜力更好地靶向使用基于紫杉烷的治疗。
英国癌症研究中心(CRUK 01/001)、赛诺菲 - 安万特、辉瑞和罗氏公司。