Berg Anne T, Levy Susan R, Testa Francine M, D'Souza Ramona
Department of Biology, Northern Illinois University, DeKalb, IL 60115, USA.
Ann Neurol. 2009 May;65(5):510-9. doi: 10.1002/ana.21642.
Determine the probability of a more than 1-year remission after failure of a second drug in children prospectively followed from initial diagnosis of epilepsy and then from time of second drug failure. Identify prognostic factors for remission after second drug failure.
Of 613 children, 128 did not respond favorably to 2 drugs, had a trial of at least a third drug (median, 3), and were followed for more than 1 year (median, 10.1 years) since second drug failure. Product limit and proportional hazards techniques were used to analyze predictors of any 1-year remission (Rem1) and 1- and 3-year remission at last contact (Rem1/3-LC).
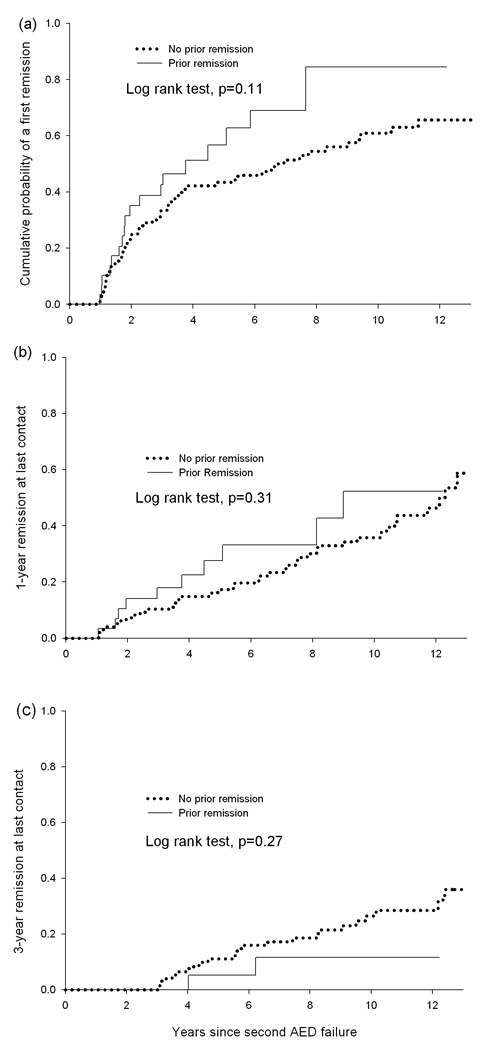
Seventy-three patients (57%) had a remission. Repeated remissions and relapses were common. Only 48 (37.5%) achieved Rem1-LC and 28 (23%) Rem3-LC. Idiopathic epilepsy (Rem1: rate ratio [RR], 3.64, p < 0.0001; Rem1-LC: RR, 2.57, p = 0.008) and seizure frequency (Rem1: RR, 0.76, p = 0.003; Rem1-LC: RR, 0.82, p = 0.04 per increase in category) were the most robust predictors. Symptomatic cause was the only correlate of Rem3-LC. Remission before second drug failure did not predict remission after second drug failure.
Remission after second drug failure is common but often temporary. Children who have not responded to two appropriate drugs should be carefully evaluated to maximize therapy and possibly considered for more aggressive treatments.
确定自癫痫初始诊断起并从第二种药物治疗失败时开始前瞻性随访的儿童,在第二种药物治疗失败后缓解超过1年的概率。确定第二种药物治疗失败后缓解的预后因素。
在613名儿童中,128名对两种药物反应不佳,接受了至少第三种药物的试验(中位数为3种),自第二种药物治疗失败后随访超过1年(中位数为10.1年)。采用乘积限界法和比例风险技术分析任何1年缓解(Rem1)以及最后一次随访时1年和3年缓解(Rem1/3-LC)的预测因素。
73名患者(57%)出现缓解。反复缓解和复发很常见。只有48名(37.5%)实现了Rem1-LC,28名(23%)实现了Rem3-LC。特发性癫痫(Rem1:率比[RR],3.64,p<0.0001;Rem1-LC:RR,2.57,p = 0.008)和发作频率(Rem1:RR,0.76,p = 0.003;Rem1-LC:RR,0.82,每增加一个类别p = 0.04)是最有力的预测因素。症状性病因是Rem3-LC的唯一相关因素。第二种药物治疗失败前的缓解并不能预测第二种药物治疗失败后的缓解。
第二种药物治疗失败后的缓解很常见,但往往是暂时的。对两种合适药物无反应的儿童应进行仔细评估,以优化治疗,并可能考虑采取更积极的治疗方法。