Department of Anesthesia, Heart Institute, Faculdade de Medicina, Universidade de São Paulo, São Paulo, SP, Brazil.
Clinics (Sao Paulo). 2009;64(4):279-85. doi: 10.1590/s1807-59322009000400003.
To evaluate the effects of intrathecal morphine on pulmonary function, analgesia, and morphine plasma concentrations after cardiac surgery.
Lung dysfunction increases morbidity and mortality after cardiac surgery. Regional analgesia may improve pulmonary outcomes by reducing pain, but the occurrence of this benefit remains controversial.
Forty-two patients were randomized for general anesthesia (control group n=22) or 400 microg of intrathecal morphine followed by general anesthesia (morphine group n=20). Postoperative analgesia was accomplished with an intravenous, patient-controlled morphine pump. Blood gas measurements, forced vital capacity (FVC), forced expiratory volume (FEV), and FVC/FEV ratio were obtained preoperatively, as well as on the first and second postoperative days. Pain at rest, profound inspiration, amount of coughing, morphine solicitation, consumption, and plasma morphine concentration were evaluated for 36 hours postoperatively. Statistical analyses were performed using the repeated measures ANOVA or Mann-Whiney tests (*p<0.05).
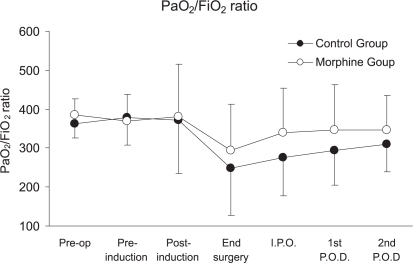
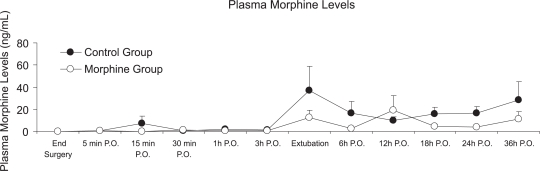
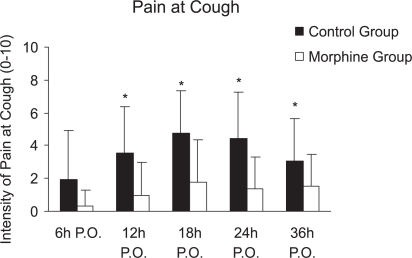
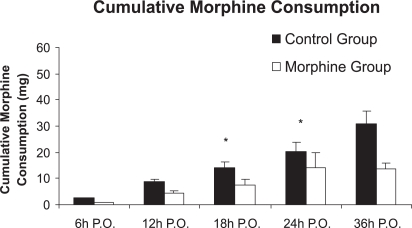
Both groups experienced reduced FVC postoperatively (3.24 L to 1.38 L in control group; 2.72 L to 1.18 L in morphine group), with no significant decreases observed between groups. The two groups also exhibited similar results for FEV1 (p=0.085), FEV1/FVC (p=0.68) and PaO2/FiO2 ratio (p=0.08). The morphine group reported less pain intensity (evaluated using a visual numeric scale), especially when coughing (18 hours postoperatively: control group= 4.73 and morphine group= 1.80, p=0.001). Cumulative morphine consumption was reduced after 18 hours in the morphine group (control group= 20.14 and morphine group= 14.20 mg, p=0.037). The plasma morphine concentration was also reduced in the morphine group 24 hours after surgery (control group= 15.87 ng.mL-1 and morphine group= 4.08 ng.mL-1, p=0.029).
Intrathecal morphine administration did not significantly alter pulmonary function; however, it improved patient analgesia and reduced morphine consumption and morphine plasma concentration.
评估鞘内注射吗啡对心脏手术后肺功能、镇痛效果和吗啡血浆浓度的影响。
肺功能障碍会增加心脏手术后的发病率和死亡率。区域镇痛可能通过减轻疼痛来改善肺功能结局,但这种益处的发生仍存在争议。
42 名患者随机分为全身麻醉组(对照组,n=22)或全身麻醉后鞘内注射 400μg 吗啡组(吗啡组,n=20)。术后镇痛采用静脉自控吗啡泵。术前及术后第 1、2 天分别进行血气测量、用力肺活量(FVC)、用力呼气量(FEV)和 FVC/FEV 比值。术后 36 小时评估静息时疼痛、深吸气时疼痛、咳嗽次数、吗啡需求、消耗和血浆吗啡浓度。采用重复测量方差分析或 Mann-Whitney 检验进行统计学分析(*p<0.05)。
两组患者术后 FVC 均下降(对照组:3.24L 降至 1.38L;吗啡组:2.72L 降至 1.18L),但组间无显著差异。两组 FEV1(p=0.085)、FEV1/FVC(p=0.68)和 PaO2/FiO2 比值(p=0.08)也有相似的结果。吗啡组报告的疼痛强度较低(采用视觉数字评分评估),尤其是咳嗽时(术后 18 小时:对照组=4.73,吗啡组=1.80,p=0.001)。吗啡组术后 18 小时累积吗啡消耗量减少(对照组=20.14mg,吗啡组=14.20mg,p=0.037)。术后 24 小时,吗啡组的血浆吗啡浓度也降低(对照组=15.87ng.mL-1,吗啡组=4.08ng.mL-1,p=0.029)。
鞘内注射吗啡并未显著改变肺功能,但改善了患者的镇痛效果,减少了吗啡的消耗和血浆浓度。