Fjerstad Mary, Trussell James, Sivin Irving, Lichtenberg E Steve, Cullins Vanessa
Planned Parenthood Federation of America, New York, USA.
N Engl J Med. 2009 Jul 9;361(2):145-51. doi: 10.1056/NEJMoa0809146.
From 2001 through March 2006, Planned Parenthood health centers throughout the United States provided medical abortion (abortion by means of medication) principally by a regimen of oral mifepristone followed 24 to 48 hours later by vaginal misoprostol. In response to concern about serious infections, in early 2006 Planned Parenthood changed the route of misoprostol administration from vaginal to buccal and required either routine provision of antibiotics or universal screening and treatment for chlamydia; in July 2007, Planned Parenthood began requiring routine treatment with antibiotics for all medical abortions.
We performed a retrospective analysis assessing the rates of serious infection after medical abortion during a time when misoprostol was administered vaginally (through March 2006), as compared with rates after a change to buccal administration of misoprostol and after initiation of additional infection-reduction measures.
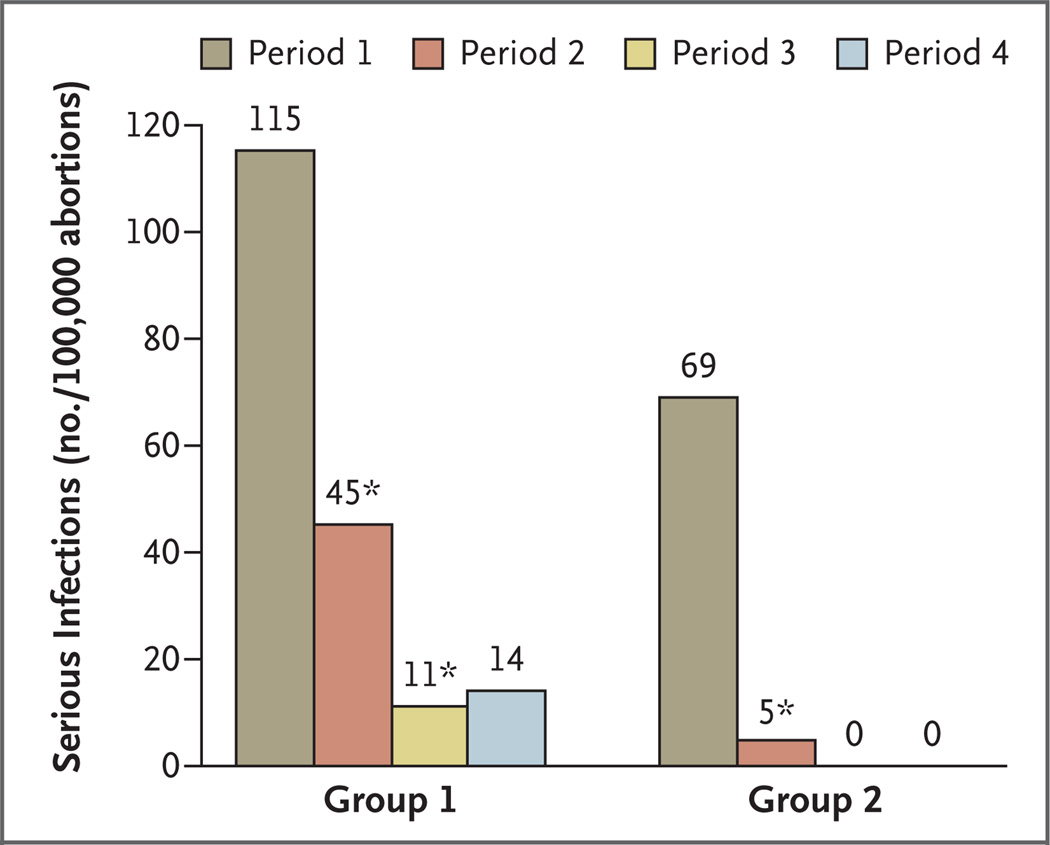
Rates of serious infection dropped significantly after the joint change to buccal misoprostol from vaginal misoprostol and to either testing for sexually transmitted infection or routine provision of antibiotics as part of the medical abortion regimen. The rate declined 73%, from 0.93 per 1000 abortions to 0.25 per 1000 (absolute reduction, 0.67 per 1000; 95% confidence interval [CI], 0.44 to 0.94; P<0.001). The subsequent change to routine provision of antibiotics led to a further significant reduction in the rate of serious infection - a 76% decline, from 0.25 per 1000 abortions to 0.06 per 1000 (absolute reduction, 0.19 per 1000; 95% CI, 0.02 to 0.34; P=0.03).
The rate of serious infection after medical abortion declined by 93% after a change from vaginal to buccal administration of misoprostol combined with routine administration of antibiotics.
从2001年至2006年3月,美国各地的计划生育健康中心主要通过口服米非司酮,随后在24至48小时后阴道给予米索前列醇的方案来提供药物流产(通过药物进行流产)。针对对严重感染的担忧,2006年初,计划生育组织将米索前列醇的给药途径从阴道改为颊部,并要求要么常规提供抗生素,要么对衣原体进行普遍筛查和治疗;2007年7月,计划生育组织开始要求对所有药物流产进行常规抗生素治疗。
我们进行了一项回顾性分析,评估米索前列醇经阴道给药期间(至2006年3月)药物流产后严重感染的发生率,并与改为米索前列醇颊部给药后以及采取了其他减少感染措施后的发生率进行比较。
在联合改变为米索前列醇颊部给药以及将检测性传播感染或常规提供抗生素作为药物流产方案的一部分后,严重感染率显著下降。发生率下降了73%,从每1000例流产0.93例降至每1000例0.25例(绝对降低0.67例/1000;95%置信区间[CI],0.44至0.94;P<0.001)。随后改为常规提供抗生素导致严重感染率进一步显著降低——下降了76%,从每1000例流产0.25例降至每1000例0.06例(绝对降低0.19例/1000;95%CI,0.02至0.34;P=0.03)。
米索前列醇从阴道给药改为颊部给药并联合常规使用抗生素后,药物流产后严重感染率下降了93%。