National Centre in HIV Epidemiology and Clinical Research, The University of New South Wales, Sydney, Australia.
HIV Med. 2010 Jan;11(1):31-9. doi: 10.1111/j.1468-1293.2009.00738.x. Epub 2009 Jul 6.
The aim of the study was to examine the rates and predictors of treatment modification following combination antiretroviral therapy (cART) failure in Asian patients with HIV enrolled in the TREAT Asia HIV Observational Database (TAHOD).
Treatment failure (immunological, virological and clinical) was defined by World Health Organization criteria. Countries were categorized as high or low income by World Bank criteria.
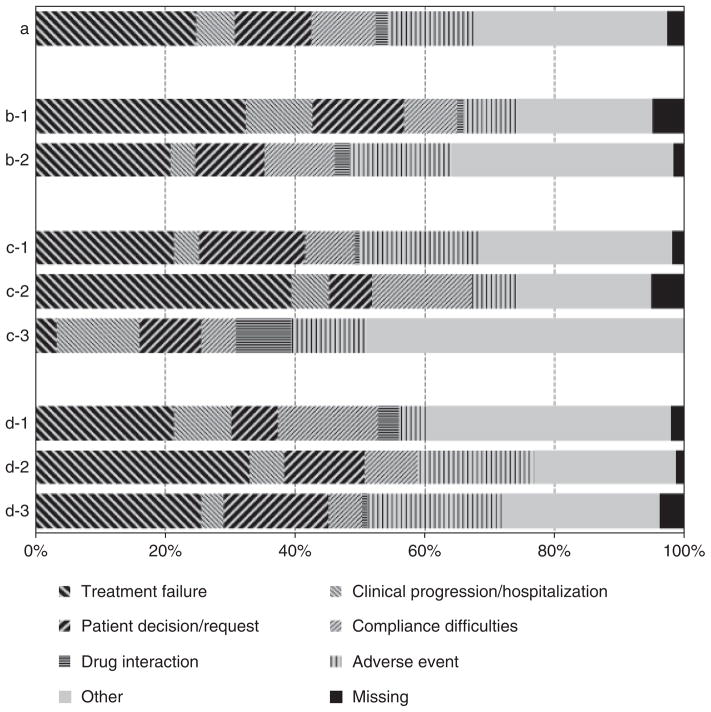
Among 2446 patients who initiated cART, 447 were documented to have developed treatment failure over 5697 person-years (7.8 per 100 person-years). A total of 253 patients changed at least one drug after failure (51.6 per 100 person-years). There was no difference between patients from high- and low-income countries [adjusted hazard ratio (HR) 1.02; P=0.891]. Advanced disease stage [Centers for Disease Control and Prevention (CDC) category C vs. A; adjusted HR 1.38, P=0.040], a lower CD4 count (>or=51 cells/microL vs. <or=50 cells/microL; adjusted HR 0.61, P=0.022) and a higher HIV viral load (>or=400 HIV-1 RNA copies/mL vs. <400 copies/mL; adjusted HR 2.69, P<0.001) were associated with a higher rate of treatment modification after failure. Compared with patients from low-income countries, patients from high-income countries were more likely to change two or more drugs (67%vs. 49%; P=0.009) and to change to a protease-inhibitor-containing regimen (48%vs. 16%; P<0.001).
In a cohort of Asian patients with HIV infection, nearly half remained on the failing regimen in the first year following documented treatment failure. This deferred modification is likely to have negative implications for accumulation of drug resistance and response to second-line treatment. There is a need to scale up the availability of second-line regimens and virological monitoring in this region.
本研究旨在考察在 TREAT Asia HIV 观察性数据库(TAHOD)中接受联合抗逆转录病毒治疗(cART)失败的亚洲 HIV 感染者中,改变治疗方案的比例及其预测因素。
根据世界卫生组织(WHO)的标准定义治疗失败(免疫学、病毒学和临床)。根据世界银行(World Bank)的标准,将国家分为高收入和低收入国家。
在 2446 名开始 cART 的患者中,447 名患者在 5697 人年(7.8/100 人年)中记录到治疗失败。共有 253 名患者在失败后至少改变了一种药物(51.6/100 人年)。高收入和低收入国家的患者之间没有差异(调整后的危险比[HR]为 1.02;P=0.891)。晚期疾病阶段[美国疾病控制与预防中心(CDC)分类 C 与 A;调整后的 HR 为 1.38,P=0.040]、较低的 CD4 计数(>或=51 个细胞/微升与<或=50 个细胞/微升;调整后的 HR 为 0.61,P=0.022)和较高的 HIV 病毒载量(>或=400 HIV-1 RNA 拷贝/ml 与<400 拷贝/ml;调整后的 HR 为 2.69,P<0.001)与失败后治疗方案改变的比例较高相关。与低收入国家的患者相比,高收入国家的患者更有可能改变两种或更多种药物(67%比 49%;P=0.009),并改变为包含蛋白酶抑制剂的方案(48%比 16%;P<0.001)。
在亚洲 HIV 感染患者队列中,近一半的患者在有记录的治疗失败后第一年仍继续使用失败的方案。这种延迟的改变可能对耐药性的积累和二线治疗的反应产生负面影响。该地区需要扩大二线方案和病毒学监测的可及性。