Social and Behvioural Sciences Unit, Public Health Sciences Division, ICDDR, B, Mohakhali, Dhaka 1212, Bangladesh.
Int J Equity Health. 2009 Aug 4;8:29. doi: 10.1186/1475-9276-8-29.
Achieving equity by way of improving the condition of the economically poor or otherwise disadvantaged is among the core goals of contemporary development paradigm. This places importance on monitoring outcome indicators among the poor. National surveys allow disaggregation of outcomes by socioeconomic status at national level and do not have statistical adequacy to provide estimates for lower level administrative units. This limits the utility of these data for programme managers to know how well particular services are reaching the poor at the lowest level. Managers are thus left without a tool for monitoring results for the poor at lower levels. This paper demonstrates that with some extra efforts community and facility based data at the lower level can be used to monitor utilization of healthcare services by the poor.
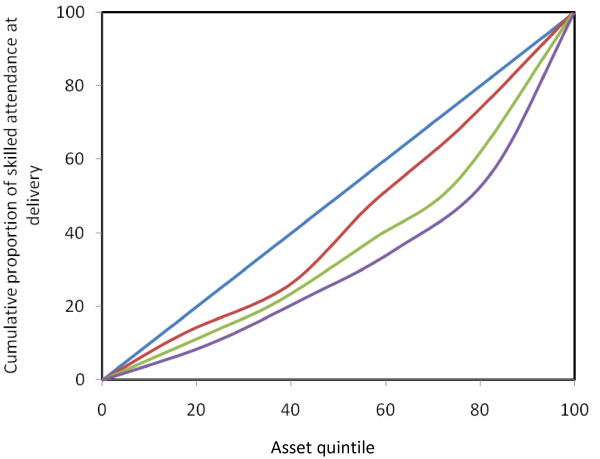
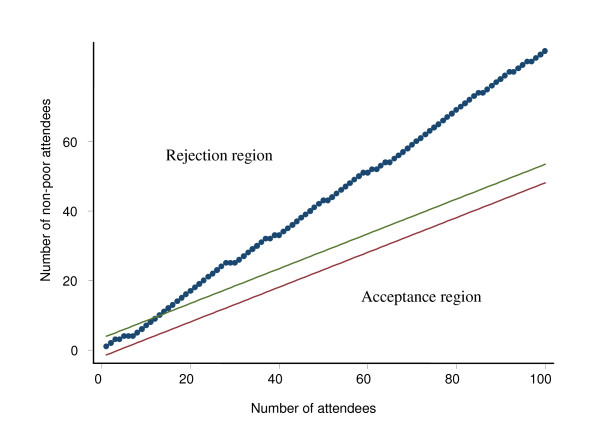
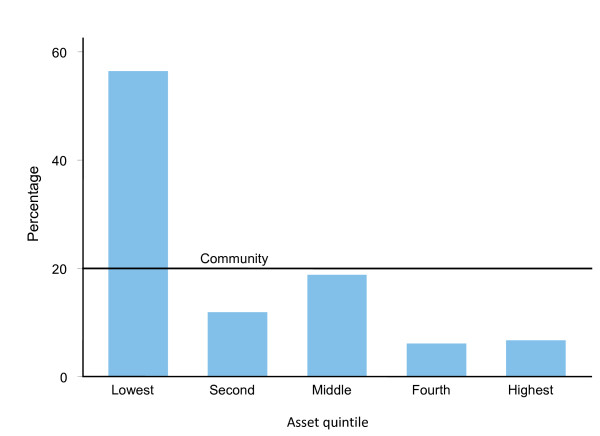
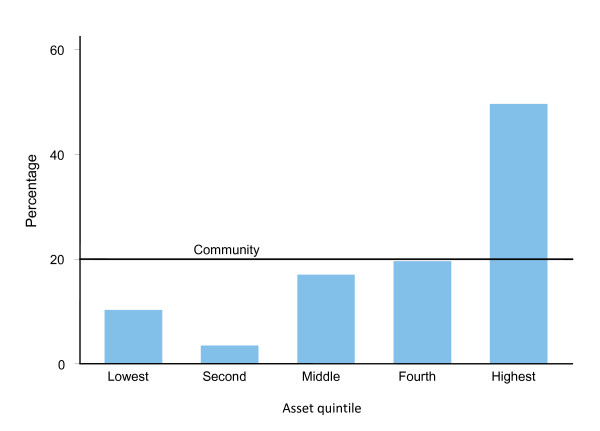
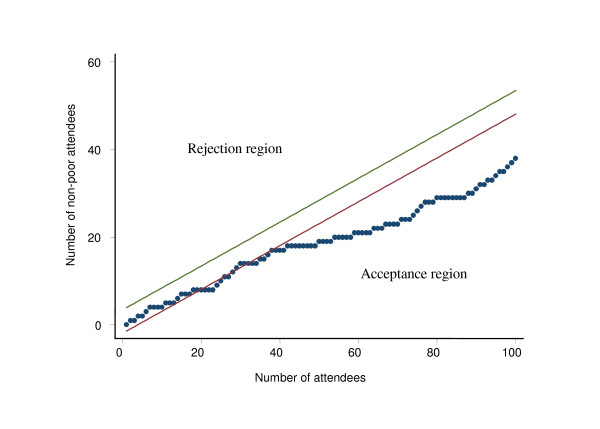
Data used in this paper came from two sources- Chakaria Health and Demographic Surveillance System (HDSS) of ICDDR,B and from a special study conducted during 2006 among patients attending the public and private health facilities in Chakaria, Bangladesh. The outcome variables included use of skilled attendants for delivery and use of facilities. Rate-ratio, rate-difference, concentration index, benefit incidence ratio, sequential sampling, and Lot Quality Assurance Sampling were used to assess how pro-poor is the use of skilled attendants for delivery and healthcare facilities.
Poor are using skilled attendants for delivery far less than the better offs. Government health service facilities are used more than the private facilities by the poor.Benefit incidence analysis and sequential sampling techniques could assess the situation realistically which can be used for monitoring utilization of services by poor. The visual display of the findings makes both these methods attractive. LQAS, on the other hand, requires small fixed sample and always enables decision making.
With some extra efforts monitoring of the utilization of healthcare services by the poor at the facilities can be done reliably. If monitored, the findings can guide the programme and facility managers to act in a timely fashion to improve the effectiveness of the programme in reaching the poor.
通过改善经济贫困或其他弱势群体的条件来实现公平,是当代发展模式的核心目标之一。这就需要关注贫困人口的结果指标。国家调查允许在国家层面上按社会经济地位对结果进行细分,但没有足够的统计能力为较低级别的行政单位提供估计值。这限制了这些数据对于方案管理者的用途,无法了解特定服务在最低级别上对穷人的覆盖程度。因此,管理者没有工具来监测较低级别穷人的成果。本文证明,通过一些额外的努力,可以利用较低级别社区和设施的数据来监测穷人对医疗保健服务的利用情况。
本文使用的数据来自两个来源—— ICDDR,B 的查卡里亚健康和人口监测系统(HDSS)和 2006 年在孟加拉国查卡里亚的公立和私立卫生设施就诊的患者进行的一项特别研究。结果变量包括熟练助产士的分娩和设施的使用。使用率比、率差、集中指数、受益发生率比、序贯抽样和批量质量保证抽样来评估熟练助产士分娩和医疗设施使用对穷人的倾斜程度。
穷人使用熟练助产士分娩的比例远远低于富裕人群。穷人更倾向于使用政府卫生服务设施,而不是私人设施。受益发生率分析和序贯抽样技术可以现实地评估情况,可用于监测穷人对服务的利用情况。调查结果的直观显示使这两种方法都具有吸引力。另一方面,LQAS 需要固定的小样本,并且总是能够做出决策。
通过一些额外的努力,可以可靠地监测穷人在设施中对医疗保健服务的利用情况。如果进行监测,这些发现可以指导方案和设施管理者及时采取行动,提高方案在覆盖穷人方面的有效性。