King Kathryn M, Norris Colleen M, Knudtson Merril L, Ghali William A
Centre for Health and Policy Studies, Department of Community Health Sciences, University of Calgary, Calgary, Alberta, Canada.
BMC Cardiovasc Disord. 2009 Aug 6;9:36. doi: 10.1186/1471-2261-9-36.
Prior research reveals that processes and outcomes of cardiac care differ across sociodemographic strata. One potential contributing factor to such differences is the personality traits of individuals within these strata. We examined the association between risk-taking attitudes and cardiac patients' clinical and demographic characteristics, the likelihood of undergoing invasive cardiac procedures and survival.
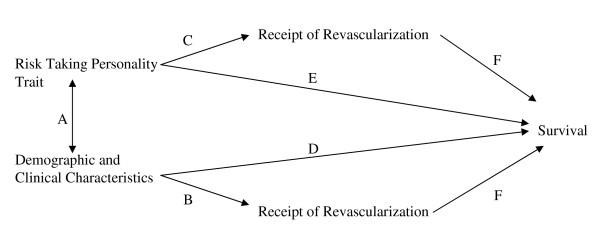
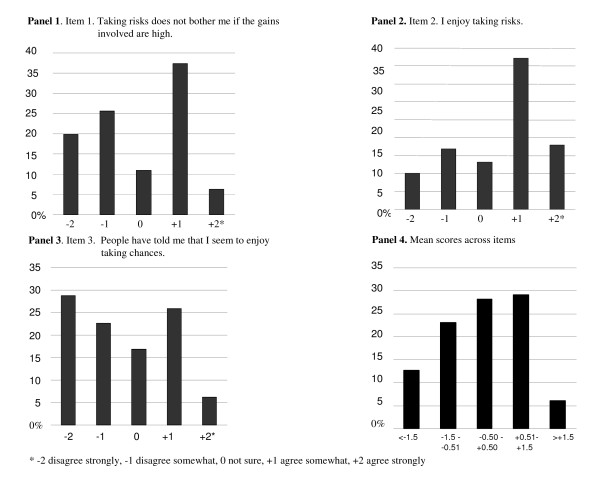
We studied a large inception cohort of patients who underwent cardiac catheterization between July 1998 and December 2001. Detailed clinical and demographic data were collected at time of cardiac catheterization and through a mailed survey one year post-catheterization. The survey included three general risk attitude items from the Jackson Personality Inventory. Patients' (n = 6294) attitudes toward risk were categorized as risk-prone versus non-risk-prone and were assessed for associations with baseline clinical and demographic characteristics, treatment received (i.e., medical therapy, coronary artery bypass graft (CABG) surgery, percutaneous coronary intervention (PCI)), and survival (to December 2005).
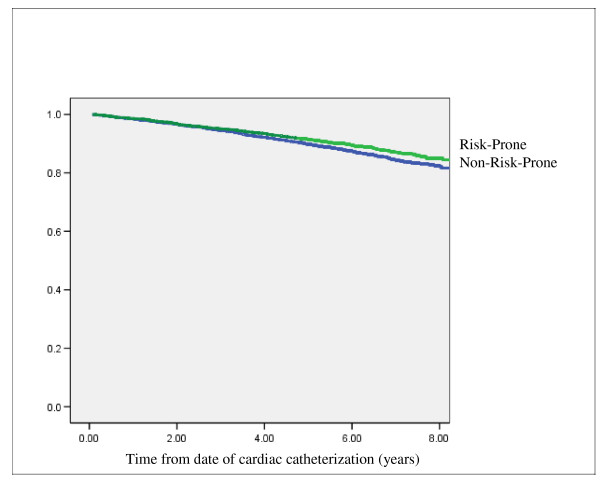
2827 patients (45%) were categorized as risk-prone. Having risk-prone attitudes was associated with younger age (p < .001), male sex (p < .001), current smoking (p < .001) and higher household income (p < .001). Risk-prone patients were more likely to have CABG surgery in unadjusted (Odds Ratio [OR] = 1.21; 95% CI 1.08-1.36) and adjusted (OR = 1.18; 95% CI 1.02-1.36) models, but were no more likely to have PCI or any revascularization. Having risk-prone attitudes was associated with better survival in an unadjusted survival analysis (Hazard Ratio [HR] = 0.78 (95% CI 0.66-0.93), but not in a risk-adjusted analysis (HR = 0.92, 95% CI 0.77-1.10).
These exploratory findings suggest that patient attitudes toward risk taking may contribute to some of the documented differences in use of invasive cardiac procedures. An awareness of these associations could help healthcare providers as they counsel patients regarding cardiac care decisions.
先前的研究表明,心脏护理的过程和结果在社会人口统计学阶层中存在差异。造成这些差异的一个潜在因素是这些阶层中个体的人格特质。我们研究了冒险态度与心脏病患者的临床和人口统计学特征、接受侵入性心脏手术的可能性以及生存率之间的关联。
我们研究了1998年7月至2001年12月期间接受心脏导管插入术的一大群初始队列患者。在心脏导管插入术时以及导管插入术后一年通过邮寄调查收集详细的临床和人口统计学数据。该调查包括来自杰克逊人格量表的三个一般风险态度项目。将患者(n = 6294)的风险态度分为倾向风险型和非倾向风险型,并评估其与基线临床和人口统计学特征、接受的治疗(即药物治疗、冠状动脉搭桥术(CABG)、经皮冠状动脉介入治疗(PCI))以及生存率(至2005年12月)之间的关联。
2827名患者(45%)被归类为倾向风险型。具有倾向风险的态度与较年轻的年龄(p <.001)、男性(p <.001)、当前吸烟(p <.001)和较高的家庭收入(p <.001)相关。在未调整(优势比[OR] = 1.21;95%可信区间1.08 - 1.36)和调整(OR = 1.18;95%可信区间1.02 - 1.36)模型中,倾向风险型患者更有可能接受CABG手术,但接受PCI或任何血运重建术的可能性并不更高。在未调整的生存分析中,具有倾向风险的态度与更好的生存率相关(风险比[HR] = 0.78(95%可信区间0.66 - 0.93)),但在风险调整分析中则不然(HR = 0.92,95%可信区间0.77 - 1.10)。
这些探索性发现表明,患者对冒险的态度可能是侵入性心脏手术使用方面一些已记录差异的原因之一。了解这些关联可能有助于医疗保健提供者在为患者提供心脏护理决策咨询时提供帮助。